Navigation
Install the app
How to install the app on iOS
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
More options
Style variation
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Covid-19 News and Discussions
- Thread starter Yommie
- Start date
Yommie
SpeedLimited
- Oct 2, 2013
- 64,193
- 37,190
- Country of Origin

- Country of Residence

- Thread starter
- #980

GTA doctor sees summer rise in COVID-19 hospitalizations
An emergency doctor in the GTA is calling for residents to get a COVID-19 booster after seeing a rise in COVID-19 hospitalizations. “I had noticed several cases of my own patients, and we had what we call a discrepancy file where all of the abnormal tests that are of significance go through and...
 toronto.citynews.ca
toronto.citynews.ca
GTA doctor sees summer rise in COVID-19 hospitalizations

The emergency sign of a Toronto hospital is photographed on Tuesday, Sept. 27, 2022. THE CANADIAN PRESS/Alex Lupul
By Afua Baah
Posted June 17, 2024 5:31 pm.
An emergency doctor in the GTA is calling for residents to get a COVID-19 booster after seeing a rise in COVID-19 hospitalizations.
“I had noticed several cases of my own patients, and we had what we call a discrepancy file where all of the abnormal tests that are of significance go through and we had seen a real increase in cases testing positive in our hospitals,” said Dr. Steve Flindall, York Region emergency physician.
Some of Dr. Flindall’s patients are considered to be in the most vulnerable group.
“All three of my cases were elderly people with significant co-morbidities, making them at high risk for complications with severe COVID.”
There have been many people in the province getting sick with what they believe might be a cold, but Dr. Flindall believes it’s likely not the common sniffles.
“Many people that I see and that I test for COVID don’t even realize that it’s still around which is a problem.”
The latest numbers show COVID-19 vaccination rates in the country are lagging. According to the Public Health Agency of Canada, 16.9 per cent of people aged five and older have had the latest booster.
“The Ontario government has stopped monitoring for COVID all together, they’re stopping wastewater testing, you are hard pressed to find home testing kits, and if you do test positive for COVID and prescribe Paxlovid, it’s becoming exceptionally hard to obtain as well,” said Dr. Flindall. “It doesn’t seem to be on many people’s radars, and unfortunately it’s causing a problem.”
Dr. Flindall said he is seeing those numbers reflected in those he recently had to treat.
“Unfortunately, none of them had been entirely up-to-date with their vaccinations and the two out of the three that needed admission hadn’t been vaccinated in over two years.”
Aside from COVID-19, doctors are also keeping an eye on other common viruses creeping back up. With school about to vacate and parents planning family trips, doctors say now should also be a good time for kids to get up to date on all their vaccinations as well.
“Europe has had a real explosion of measles in the last year and almost all of the cases we’re seeing in Canada are related to travel,” said Dr. Flindall.
According to Public Health Ontario, immunization rates for seven-year-olds have dropped considerably over recent years. In 2019-20, vaccination for measles, mumps and polio was at roughly 85 per cent. In 2021-22, those numbers plummeted to 52 per cent.
“And a lot of children fell behind on their vaccination schedules during COVID and they’re still not caught up,” said Dr. Flindall.
As for getting caught up with vaccinations this summer, especially when it comes to COVID-19, Dr. Flindall says we shouldn’t leave it to chance and the province needs to improve public health messaging in order to encourage more people to roll up their sleeves.
“It’s really endemic, there’s really not a lot of seasonality to COVID. If you’re elderly or immunosuppressant, your dependence on previous vaccinations and previous infections is not reliable at all.”
Yommie
SpeedLimited
- Oct 2, 2013
- 64,193
- 37,190
- Country of Origin
- Country of Residence
- Thread starter
- #981

Kansas sues Pfizer over 'misrepresentations' and 'adverse events' of COVID-19 vaccine
The State of Kansas has filed a lawsuit against Pfizer, Inc. for alleged consumer protection violations related to the company's manufacturing of the COVID-19 vaccine.
 www.foxbusiness.com
www.foxbusiness.com
Published June 17, 2024 11:18am EDT
Kansas sues Pfizer over 'misrepresentations' and 'adverse events' of COVID-19 vaccine
Kansas AG Kris Kobach alleges Pfizer violated the state's Consumer Protection Act
By Brianna Herlihy FOXBusinessPfizer chairman and CEO Albert Bourla: Our oncology drugs will be blockbuster ones
Pfizer chairman and CEO Albert Bourla breaks down the company's revenue on ‘The Claman Countdown.’FIRST ON FOX: The state of Kansas has filed a lawsuit against pharmaceutical company Pfizer, Inc. for alleged consumer protection violations related to the company's manufacturing of the COVID-19 vaccine, saying the company marketed the shot as "safe" even though it "knew" the vaccine was connected to "serious adverse events."
"Pfizer misled the public that it had a ‘safe and effective’ COVID-19 vaccine," the 69-page lawsuit filed Monday in the District Court of Thomas County alleges.
"Pfizer said its COVID-19 vaccine was safe even though it knew its COVID-19 vaccine was connected to serious adverse events, including myocarditis and pericarditis, failed pregnancies, and deaths. Pfizer concealed this critical safety information from the public," the suit alleges.
"Pfizer said its COVID-19 vaccine was effective even though it knew its COVID-19 vaccine waned over time and did not protect against COVID-19 variants. Pfizer concealed this critical effectiveness information from the public," it says.
COVID VACCINE COMPANIES TOLD TO FOCUS ON KP.2 VARIANT FOR FALL SHOTS, PER FDA ANNOUNCEMENT
Exterior view of the Pfizer headquarters building on Jan. 29, 2023 in New York City. (Kena Betancur/VIEWpress / Getty Images)
The lawsuit alleges that the company's "actions and statements relating to its COVID-19 vaccine" violated the Kansas Consumer Protection Act, "regardless of whether any individual consumer ultimately received Pfizer’s COVID-19 vaccine."
"Pfizer must be held accountable for falsely representing the benefits of its COVID-19 vaccine while concealing and suppressing the truth about its vaccine’s safety risks, waning effectiveness, and inability to prevent transmission," the lawsuit says.
The suit, filed by Republican Attorney General Kris Kobach, alleges that through the company's "misrepresentations" of the vaccine, it earned "record company revenue" of approximately $75 billion in just two years.

LARGEST-EVER COVID VACCINE STUDY LINKS SHOT TO SMALL INCREASE IN HEART AND BRAIN CONDITIONS

Vials with Pfizer-BioNTech and Moderna COVID vaccine labels are seen in this illustration picture taken March 19, 2021. (REUTERS/Dado Ruvic/Illustration / Reuters Photos)
The lawsuit alleges that "millions of Kansans heard Pfizer’s misrepresentations about its COVID-19 vaccine."
"For example, Pfizer administered 3,355,518 Pfizer vaccine doses in Kansas as of February 7, 2024. This accounted for more than 60% of all vaccine doses in Kansas," the lawsuit alleges, citing the state's Department of Health Data.
The lawsuit alleges that Pfizer used various methods to "conceal critical data" related to the "safety and effectiveness" of the vaccine, including using confidentiality agreements, an extended timeline, and destroying the control group participating in its vaccine trial.
"Because Pfizer unblinded the original control group and allowed them to receive Pfizer’s COVID-19 vaccine, Pfizer, government regulators, and independent scientists cannot fully compare the safety and efficacy of Pfizer’s COVID-19 vaccine against unvaccinated individuals," the lawsuit alleges.
"Pfizer’s extensive and aggressive efforts to keep its COVID-19 vaccine information hidden conflict with its public transparency pledges and raise serious questions about what Pfizer is hiding and why it is hiding it," it says.
The lawsuit also alleges that Pfizer failed to disclose the limitations of its COVID-19 vaccine trials.
CDC RECOMMENDS ADDITIONAL COVID VACCINE FOR ADULTS 65 AND OVER

Albert Bourla attends The New York Times DealBook Online Summit on Nov. 9, 2021, in New York City. (Ryan Muir/Getty Images via The New York Times / Getty Images)
"When Pfizer announced that the FDA had authorized Pfizer’s COVID-19 vaccine for emergency use, Pfizer did not disclose that its trial included only healthy individuals and excluded unhealthy individuals," the suit claims.
"Pfizer made representations about its COVID-19 vaccine’s safety knowingly or with reason to know that it did not possess a reasonable basis to represent that it was safe for individuals who had been diagnosed with COVID-19, who were immunocompromised, or who were pregnant or breastfeeding," it alleges.
The suit also claims that Pfizer had knowledge of "safety issues" with the COVID-19 vaccine.
CLICK HERE TO GET THE FOX NEWS APP
Kobach alleges that Pfizer maintained its own adverse events database, separate from the Vaccine Adverse Event Reporting System (VAERS) system, that "contain[ed] cases of [adverse events (AEs)] reported spontaneously to Pfizer, cases reported by the health authorities, cases published in the medical literature, cases from Pfizer-sponsored marketing programs, non-interventional studies, and cases of serious AEs reported from clinical studies regardless of causality assessment."
"Upon information and belief, Pfizer’s adverse events database contained more adverse event data than VAERS because it included both information in VAERS and information not in VAERS," the lawsuit alleges.
"Pfizer did not publicly release adverse events data from its database," Kobach claims.
In a statement to Fox News Digital, Pfizer said: "We are proud to have developed the COVID-19 vaccine in record time in the midst of a global pandemic and saved countless lives. The representations made by Pfizer about its COVID-19 vaccine have been accurate and science-based. The Company believes that the state’s case has no merit and will respond to the suit in due course."
"Pfizer is deeply committed to the well-being of the patients it serves and has no higher priority than ensuring the safety and effectiveness of its treatments and vaccines. Since its initial authorization by FDA in December 2020, the Pfizer-BioNTech COVID-19 vaccine has been administered to more than 1.5 billion people, demonstrated a favorable safety profile in all age groups, and helped protect against severe COVID-19 outcomes, including hospitalization and death," the company said.
"Patient safety is our number one priority, which is why we follow diligent safety and monitoring protocols," it added.
Yommie
SpeedLimited
- Oct 2, 2013
- 64,193
- 37,190
- Country of Origin
- Country of Residence
- Thread starter
- #982
Kids are losing 'huge chunks' of their childhood to long COVID. Too many are being told it's 'all in their head'
They're losing their formative years to this debilitating disease. But for too many children with long COVID, finding help is a frustrating and traumatic process that leaves them feeling isolated and invisible.
 www.abc.net.au
www.abc.net.au
Too many children with long COVID are suffering in silence. Their greatest challenge? The myth that the virus is 'harmless' for kids
By Hayley GleesonPosted Sat 15 Jun 2024 at 3:00pmSaturday 15 Jun 2024 at 3:00pm, updated 14h ago14 hours ago
If the plight of adults with long COVID remains poorly understood, the millions of children who have it worldwide are practically invisible.(ABC News: Nash Weerasekera)
abc.net.au/news/children-with-long-covid-dismissed-doctors-myth-virus-harmless/103959078
Copy linkLink copied
Share article
Before she got sick with long COVID, Vivien* was at the top of all of her classes at school. She loved playing basketball and netball and running around with her dogs — she'd even take herself for runs around her family's sprawling property in regional New South Wales, just for fun. She's still only 12 but for the longest time Vivien has dreamed of being a vet when she grows up. "And she was so social," her mother Katie* says. "My husband and I are both introverts. Not V — she would party every day if she could."
Now, two years since she caught SARS-CoV-2 for the first time, a "good day" for Vivien looks nothing like it used to. She's always exhausted, but her achy limbs might feel less tingly and weak; perhaps her upset stomach is calm, and her brain fog has cleared enough that she can do some school work or call a friend. On a really good day, she can manage a visit with her grandparents, so long as she's prepared to spend the evening in bed. "Long COVID makes my body feel weak," Vivien says. "But I tell myself I am still powerful."
She's strong because she has to be. Like many kids with long COVID Vivien has seen a dizzying number of doctors, not all of whom have believed or helped her. She's made the tricky transition to homeschooling, learned to manage her turbulent symptoms with pacing and medication, cried fat tears of frustration after doing too much and wiping herself out.
"I want people to know that I'm not lying, [long COVID] is real and can happen to anyone," Vivien says. "I want people to know I'm not just trying to get out of doing school or sport — I wish I could do sport … I wish they understood I am just trying to save myself from being stuck in bed in pain for days afterwards."
Long COVID will take your health, your wealth — then it will come for your marriage
Long COVID is not just destroying people's health. Behind closed doors, in homes across Australia and abroad, it is irreversibly changing relationships — sometimes for the better, too often for worse.Read more
More than four years after the first COVID patients began raising the alarm that they weren't getting better, scientists are still racing to unravel the mystery of why a significant minority of people develop debilitating chronic symptoms while others seem to recover just fine. But if the plight of adults with long COVID remains poorly understood, the millions of children who have it worldwide are practically invisible, their suffering — and the formative years they're losing to this disease — obscured by the myths that COVID is "harmless" for kids and the pandemic is "over".
In Australia, the lack of awareness is biting in shocking ways. Too many children with long COVID are being dismissed by doctors who say there's nothing they can do to help — or worse, that their pain and fatigue is "all in their head". They're being pushed out of school by teachers who don't understand why they can't come to class or run around with their peers. Their parents have been gaslighted and blamed, too, not just by medical professionals but their closest friends and family. And experts are concerned that all this ignorance and apathy — and the unwillingness of governments to do more to curb COVID transmission — is exposing a generation of children to the same chronic illness and disability, with potentially devastating consequences.
"These kids' worlds just get very small, very quickly," says David Putrino, who runs a long COVID clinic as director of rehabilitation innovation for the Mount Sinai Health System in New York. "We see kids missing school, being unable to participate in sports, we see social isolation." Long COVID is "a lot more complicated and more brutal" for young people, he says — adults tend to be better able to navigate the medical intricacies and politics of their illness. "I don't like comparative suffering as a concept … but I do know that … kids are having a harder time with it because people seem to be less understanding of it."
A crucial reason paediatric long COVID has been overlooked is that children generally suffer less severe acute infections than adults. Governments and public health agencies have also been "pushing the narrative" that the only negative possible outcome of catching COVID is death, Dr Putrino says. "We looked at the acute phase and said, 'This doesn't seem so bad for kids', and we forgot about the cumulative risks over time." It doesn't matter how mild your acute COVID infection is, he says: "You have the same risk of developing long COVID. And I say 'cumulative' because the latest data shows us that with every reinfection, your risk of long COVID increases."
What does long COVID look like?
Getting a handle on the scale of the problem is difficult because prevalence estimates of long COVID in children vary widely, though many researchers believe it likely affects 1–5 per cent of kids who catch the virus. While some experts have argued it is "rare" and not a concern for most families, others insist even 1 per cent is significant given huge swathes of the population are getting (re)infected — and the impacts of long COVID are so severe. In the UK, for instance, the number of children reporting they have long COVID almost doubled in the year to March 2024, with nearly one in five revealing their symptoms limited their ability to undertake day-to-day activities "a lot".As for what it looks like, long COVID can affect multiple organ systems and trigger a constellation of symptoms that can last for months or years: the most common are fatigue, including post-exertional malaise (PEM) or "crashing" after even light activity; cognitive dysfunction and headaches; gastrointestinal issues and allergic reactions; nerve and muscle pain; dysautonomia; and shortness of breath. These symptoms overlap with those of myalgic encephalomyelitis/chronic fatigue syndrome, to the extent that many long COVID patients meet ME/CFS diagnostic criteria, their fatigue and PEM stopping them from living their normal lives well beyond six months.
And if the causes of long COVID sound complex, it's because they are. Researchers have zeroed in on several likely mechanisms, including viral persistence; inflammation and immune dysregulation; blood clotting and coagulation issues; organ damage; autoimmunity; reactivation of latent viruses like Epstein-Barr; and disrupted brainstem signalling.
Still, there is a serious lack of research on long COVID in children, particularly in Australia, which is concerning because, as a parliamentary inquiry last year heard, young people may be at greater risk of repeated infections as they spend so much time in crowded spaces like schools, and they have lower rates of vaccination than adults.
One of the greatest challenges children with long COVID and their families are grappling with is not knowing when or if they'll recover.(ABC News: Nash Weerasekera)
But identifying these kids in the first place can be challenging, raising concerns many are being missed or misdiagnosed. Doctors say it's common for children to present initially with gastrointestinal issues — complaints of an upset stomach, usually — and only with careful questioning does the full picture of their illness become clear. "It's surprising how profoundly long COVID can impact a child's life, and how much inquiry you have to do to actually work that out," says Michelle Scoullar, a Melbourne-based paediatrician at Clinic Nineteen, a specialist practice that sees long COVID patients by telehealth.
Because Dr Scoullar's patients are so resilient, she says, they'll often tell her at the start of an appointment that they're "doing okay", maybe even improving. But with deeper probing she'll discover that "okay" is anything but: they're not just struggling to get to school, they don't have the energy to get to the bathroom by themselves. "Improving" by their standards might mean they were able to spend 20 minutes at the dinner table one evening, but pretty much the rest of the week on the sofa or in bed. "We've got kids missing out on large chunks of their childhood," she says. "And the social, developmental and educational impacts of that can last years."
One of the things that shocks Dr Scoullar most, though, is how many of her patients have struggled with other doctors, especially paediatricians. Instead of kindness and support, she says, "They get judgement, ignorance and not just unhelpful advice, but incorrect and harmful advice. Many of the children I have seen have been told to just rest up, try a bit harder, get back to exercise. They're told, 'You're not doing enough and that's why you're feeling so tired'," she says. "And that's just completely unacceptable."
When doctors harm, not help
Katie learned that the hard way, riding a "rollercoaster of GPs" in the months after Vivien fell ill. The "biggest problem" is that many GPs don't understand what long COVD is, she says, and some are reluctant to refer to specialists.The first GP they saw told Katie that "kids don't get long COVID" so she should just keep an eye on Vivien. Another listened as she explained her daughter's symptoms and insisted there was nothing wrong, it was "just a bad respiratory season". "We need to educate GPs because they're gatekeepers," Katie says. "Once we found a GP who was humble enough to admit she didn't know what was happening, things got better."
But specialists weren't much help, either. One of the two times Katie has cried about a doctor was after an appointment with a paediatric neurologist in Sydney, who she hoped would have answers for Vivien's headaches and lost sense of smell. Instead, the doctor shrugged and said there was nothing much she could do, just give it more time. Katie was stunned; she'd waited eight months and paid nearly $800 for the appointment — she didn't need counselling on patience. "That was the day that broke me," she says. "We were walking back to the car, four hours from home, and I just could not stop crying. I desperately wanted that neurologist to be part of the solution. If we could just fix the headaches…"
Dee feels like a prisoner in her own body and wants more people to know the truth about her illness
People with myalgic encephalomyelitis, also known as chronic fatigue syndrome, say society has long underestimated and downplayed their struggles.Read more
Mark Donohoe hears stories like these every week. An integrative GP who has been treating people with ME/CFS for 40 years, Dr Donohoe says a common stumbling block for kids with long COVID is that standard blood tests will often come back normal and many GPs and paediatricians don't know to check for postural orthostatic tachycardia syndrome (POTS), a type of dysautonomia common among long COVID patients that can cause a rapid increase in heart rate on standing, dizziness, headaches and fatigue. Delays in getting diagnosed can be costly, he says. "The longer you've been sick, the longer it takes to recover function."
But because research on long COVID is still emerging, time-poor doctors can lose their curiosity about what's happening for their patients, Dr Donohoe says, not realising supplements, medication and lifestyle interventions can dramatically improve their quality of life. They'll say, "It's long COVID, the official answer is there's nothing to do," he says. "And they tell the parents, 'Just get them up and get them active' — and that's the advice that really exacerbates things." Because if a child who suffers from post-exertional malaise (PEM) is pushed beyond their capacity, they can deteriorate rapidly.
Crucially, PEM isn't "normal" fatigue; it's not just feeling tired after a big day or a sign a child is out of shape. It's a worsening of symptoms after physical or cognitive activity — a failure of the immune system and metabolism to meet energy demands. It also looks different in every patient: some can't brush their teeth without triggering it, while others might be able to get to school but then suffer a crash that lasts for days as a result. And for many people with long COVID and ME/CFS, exercise is a sure-fire way to provoke PEM, which is why clinical guidelines in the US and UK advise doctors not to recommend it without strict supervision.
Australian guidelines seem to be stuck in the past. The current clinical guidelines have faced sustained criticism for promoting graded exercise therapy since they were published in 2002. And the Royal Australian College of General Practitioners' new guidance on incremental physical activity for ME/CFS points to the controversial PACE trial — a 2011 study that claimed patients who did graded exercise and psychotherapy made impressive recoveries — but does not mention its methodology was found to be flawed and its findings exaggerated.
RACGP President Nicole Higgins says the guide clearly states that "this approach will not be suitable for all patients" and "does not purport to be a guideline for the comprehensive management" of ME/CFS. But patients and advocacy groups have argued it ignores the science of PEM and downplays the risk of harm to people who suffer it.
RACGP President Nicole Higgins.(Supplied: Nicole Higgins)
Graded exercise therapy can be appropriate for some children with long COVID who may have lost fitness and strength after catching the virus, says Todd Davenport, a physical therapist and exercise scientist at the University of the Pacific in California. But "it really takes a clinician who is familiar with long COVID to first determine when working out will not work out".
Instead of guiding patients to exercise, Dr Davenport says, GPs should first establish whether PEM is a problem, then look at treating its underlying causes. "I always suggest referring to experts who are in the best position to help the patient and also to support the GP," he says. If they determine that exercise could be helpful, he says, it should be closely monitored to avoid triggering PEM.
Aside from prescribing unqualified exercise, Dr Donohoe says one of the "worst" decisions a doctor can make about a child with long COVID is that there's nothing wrong with them and "they need to see a psychologist". For one thing, it ignores the thousands of peer reviewed studies documenting the disease processes of long COVID. But it's a pivotal moment, he says, "where what we're really saying in medicine is, 'We haven't got a clue what's going on … but this may make you feel better'. I think that's the point where [conditions like long COVID and ME/CFS] get converted into a psychological or psychiatric disorder."
It's not just 'all in your head'
Sometimes that conversion happens terrifyingly fast. For three months after Jack* caught COVID last May he was in and out of the emergency department at a Perth hospital with 10 out of 10 stomach pain and fatigue so crushing he couldn't walk.Now aged 13, Jack was a fit and talented athlete whose life revolved around sports, especially cricket, rugby and tennis. It's a major reason his father Brett* was so shocked when, during one of their visits to the hospital, a neurologist performed a few reflex tests on Jack, concluded his nerves were fine, then announced his symptoms were psychological.
"He said, 'Listen, it's all in your son's head, he has something called FND — functional neurological disorder'," says Brett. "I said, 'Is that psychosomatic?' and he said, 'Well, we don't call it that anymore'." Brett now knows that FND is a controversial diagnosis that should only be made after excluding other possible medical conditions. Numerous long COVID patients have reported being misdiagnosed with FND — a precarious situation, experts say, because it can block their access to testing and treatment. But Jack was devastated. "He was crying because he's the kid who goes to rugby with a migraine … he'll push through anything," Brett says. "So for the neurologist to say … it was all in his head, I think that broke him a bit."
Long COVID can affect multiple organ systems and trigger a constellation of symptoms that can last for months or years.(ABC News: Nash Weerasekera)
A couple of months later, having dug deep into the research on long COVID, Brett took Jack to Europe, where he underwent several cycles of an expensive blood filtering treatment called H.E.L.P. apheresis. The enormous cost — about $30,000 all up — should have ruled the trip out, but with the generous support of family and friends, they raised enough money to go.
Brett felt sure it was the best next step; taking vitamins and supplements helped Jack to a point, but his progress had stalled, and local doctors weren't offering anything other than paracetamol. "We were reaching the six-month mark and I knew we had to act quickly," Brett says. "[Jack] is a really, really good sportsman, I didn't want him to live with a disability."
For long COVID patients, apheresis involves removing the blood, filtering it of SARS-CoV-2 spike proteins and so-called microclots that may be clogging capillaries and stopping oxygen from getting to tissues, then returning it to the body. The microclot hypothesis as a driver of long COVID remains just that, and some experts have warned there is little published evidence showing apheresis is an effective treatment. While some patients say it has helped them almost fully recover, others have reported it made no difference or in some cases made them worse, so those who decide to have it are gambling that it will work.
Jack made a remarkable recovery. "I got a lot better — like, 90 per cent better," he says. "I was able to play tennis and go surfing and all of that." He's since suffered a disappointing relapse but his symptoms aren't as bad as they were before apheresis. In all, it was a positive experience, says Brett, who is "seriously considering" another trip overseas.
Still, he's frustrated that he felt forced to pursue an unapproved treatment on the other side of the world — and that most doctors' understanding of long COVID lags so far behind the science. "It's been really tough to sit on the margins of what people think is conspiracy and what is science and logic," he says. "Even some of my closest friends have been fighting me on it … unwilling to engage in the conversation, simply because it went against the narrative."
Struggling at school
But then ignorance and judgement can often be found in the most unlikely places. Leah's* son Sam* had been struggling with long COVID and POTS for about six months when his Sydney public high school rang her to say he wasn't meeting attendance requirements and would need to switch to distance education.At that point Sam was pushing himself to get through two or three classes a day, even though it seemed to be making him sicker — he was desperate not to fall behind academically and, like most teenagers, loved spending time with his friends. "His number-one goal is just to be back at school," Leah says. But although his doctors have provided medical certificates, "the whole way along the school has acted suspiciously, as if he's just avoiding school for the sake of it."
One complicating factor is that Sam often appears fine — there's a reason complex chronic conditions like long COVID and ME/CFS are called "invisible" illnesses. Other people don't realise that basic activities drain his energy and flare his symptoms, says Leah, who quit her full-time job to look after him. "Just going up the stairs is hard, he can't shower every day, and when he's not at school he spends most of his time in bed. But if someone comes for a quick visit he can still be pretty witty — he masks his symptoms so well — so they assume he's fine."
Even close family and friends don't truly get it. "We've been told that COVID is over and everyone just wants to ignore it and pretend it's not there," Leah says. "If it was cancer, people would be checking in and have some level of understanding. But long COVID is this slightly difficult topic that everyone avoids."
Kids with long COVID are being made to do vigorous exercise in PE class, urged to stay at school longer than their doctors advise, and refused special provisions for exams.(ABC News: Nash Weerasekera)
After deciding that distance education wasn't going to suit Sam — and that his school's attempt to push him out was "totally inappropriate" — Leah was on the phone to one of the principals one day when she casually mentioned that she'd sought legal advice to better understand their options. "It was like I'd dropped a bomb," she says. They were suddenly happy to make accommodations and allow Sam to keep coming on a reduced schedule, she says — one lesson a day.
Things have since calmed down, but for a while Sam's teachers kept pushing him to try harder, to do more, Leah says, which just piled on even more pressure. "They also didn't properly brief all his teachers. At one stage one suggested in front of the whole class that he was just acting like a bit of a rebel."
Accounts like these are disturbingly common: parents in several states say kids are being made to do vigorous exercise in PE class, urged to stay at school longer than their doctors advise, and refused special provisions for exams. In Dr Donohoe's experience, public schools are generally better than private schools at supporting young people with long COVID and ME/CFS, even in simple ways like finding them quiet spaces to lay down and rest when they need to.
Dr Scoullar has noticed similar patterns. Too often her long COVID patients tell her that their inability to get to school or stay for a full day is "a barrier that schools are very unwilling to work around", she says. "And I have heard of at least a few children who have been asked to leave because they are no longer meeting the school's requirements."
For some students, shifting to distance education is a positive change because it gives them more control over their time and energy. But Sam wouldn't have coped well with the social isolation. "The whole thing has been utterly devastating on so many levels," Leah says of her son's illness. "I'm grieving for the life that he's lost and the life he should be living, because he's missing his teenage years. And I try to be positive; I do believe he can recover. But there are just so many unknowns and so many battles — I'm constantly in battles with the school, to get medical letters, and continually having to advocate for him."
Fears for the future
It's one of the greatest challenges children with long COVID and their families are grappling with: not knowing when — or if — they'll recover. Tied to that is the financial pressure so many parents are under: between healthcare appointments, medication and supplements, some are stretching their budgets to spend hundreds or thousands of dollars every month in hopeful bids to get their kids well.For others who can barely afford to buy groceries, just getting to a GP is out of the question, so thinking about the future is frightening. "You live with this fear of, what's going to happen? What if I have a heart attack or lose more function," says Amy*, who has two kids with ME/CFS and long COVID and also has long COVID herself. "Probably my biggest fear is that this is life from now on."
Some children do recover over time, says Dr Putrino, whose clinic recommends various different therapeutic approaches: autonomic rehabilitation strategies like breathwork and gentle exercise to calm and regulate the nervous system, pacing to manage energy levels, and medication and supplements to target particular symptoms. "In other cases we struggle. Unfortunately, we have a handful of bed-bound patients … that no matter what we try, we just can't seem to move the needle," he says. "And so we just do what we always do with any patient — whether it be a stroke, or a traumatic brain injury or a long COVID adult — we say, 'We're here with you, and we're going to keep trying different things, there's lots of different things to try, and we're just going to try and find the balance'."
"I just worry we're going to have a generation of kids who have a post-acute infection syndrome because we failed to protect them," says Dr David Putrino.(Supplied)
While the world waits for clinical trials to shed light on effective treatments, patients say doctors must get up to speed on long COVID — at a minimum, GPs need comprehensive guidelines and training on how to diagnose and help patients manage their illness. The final report of Australia's parliamentary inquiry into long COVID recommended the same.
In its response, however, the government merely acknowledged the critical role of primary care providers and did not commit any additional resources for addressing the issues raised. RACGP President Nicole Higgins says funding for the National Clinical Evidence Taskforce's COVID guidelines has also been discontinued. "The RACGP has advocated for government funding for the establishment of living guidelines across a range of topics," she says, "and this is a case study for why such funding is so necessary."
Some experts are also concerned about Australia's COVID vaccine strategy given evidence suggests that vaccination reduces the risk of long COVID, including in young people. The Australian Technical Advisory Group on Immunisation (ATAGI) has previously recommended children aged five and over receive a primary course but now recommends that those under 18 not be vaccinated unless they are at increased risk of severe disease.
"ATAGI's current recommendations … acknowledge that overall, severe COVID-19 in children is extremely rare, even among unvaccinated children and those with underlying conditions," a spokesperson for the Department of Health told ABC News. "ATAGI will continue to monitor and review all emerging evidence on the use of COVID-19 vaccines, including the emerging evidence on long COVID as appropriate."
The COVID-safe strategies Australian scientists use to protect themselves from the virus
Three of Australia's leading COVID-19 experts share their personal safety strategies and reflect on what must happen if we're to blunt the growing health crisis the pandemic is causing — and prepare for the next one.Read more
For Dr Putrino, one of the biggest hurdles remains the misconception that children don't suffer long-term consequences after catching the virus. "I think that there's an enormous amount of education that needs to happen to inform parents that yes, your kid can get long COVID. Yes, it could be the reason why they're struggling in school right now," he says. "Get it checked out — don't sit around and just assume that they're going through puberty or they're just extra moody; don't sleep on it. Make sure that a doctor evaluates them. Make sure it's a doctor that's knowledgeable and educated about long COVID."
He also worries that not enough is being done to prevent COVID transmission in the community, particularly in schools. Governments could be scrambling to improve indoor air quality with good ventilation, air purifiers and far UV light, he says. But for the most part their approach has been to just let the virus rip — and watch the numbers of people with long COVID rise. "I just worry we're going to have a generation of kids who have a post-acute infection syndrome because we failed to protect them," Dr Putrino says, "because we told this lie over and over again that kids have nothing to worry about with COVID."
It's one of the things Katie is most angry about: that Vivien caught COVID at school before she was able to be fully vaccinated. Her quality of life has improved "out of sight" in the two years since then, she says, largely because they finally found a compassionate paediatrician and a couple of other specialists who understand her illness, who want to help.
"But I can see a world where I'd have to be a full-time carer," she says. "That's the thing that's really starting to scare me, is: what does the future look like? All V wants to do is be a vet — that's all she's wanted since she was five. But what if she can't? I'm trying to make decisions about our finances now so that we can help her in the future, because I can't imagine that she's ever going to get back to 100 per cent, at least not at this trajectory."
And that, she says, is what most people fail to understand about long COVID: how serious it is, how much is at stake — how fast a healthy girl with boundless energy and big dreams can lose it all. "They think it's incredibly rare, or they don't understand that just because you had one 'nice' bout of COVID doesn't mean the next one isn't going to do permanent damage," Katie says. "People just underestimate it; they assume it won't happen to them and if it does, that someone will be there to help them."
*Names have been changed at families' request so they could speak frankly without fear of reprisal.
Posted 15 Jun 202415 Jun 2024, updated 14h ago
Yommie
SpeedLimited
- Oct 2, 2013
- 64,193
- 37,190
- Country of Origin
- Country of Residence
Yommie
SpeedLimited
- Oct 2, 2013
- 64,193
- 37,190
- Country of Origin
- Country of Residence
- Thread starter
- #984
Weekly case numbers from around Australia: 12,309 new cases ( 12%)
12%)
Australia: Case Update- NSW 5,048 new cases (9%)
- VIC 2,581 new cases (
 3%)
3%) - QLD 2,238 new cases (1%)
- WA 471 new cases (35%)
- SA 1,548 new cases (37%)
- TAS 133 new cases (6%)
- ACT 189 new cases (29%)
- NT 101 new cases (24%)
")
Note that there may be slight under-reporting this week due to King's Birthday public holiday in NSW, Vic, SA, Tas, ACT, and the NT. However all indicators are suggesting that we are close to, or past, the peak now with decreasing hospitalisation rates in NSW, VIC and QLD, plus slightly lower wastewater rates in VIC and WA.
Flu tracker tracks cold and flu symptoms (fever plus cough) and is another useful tool for tracking the level of respiratory viruses in the community. This decreased slightly to 2.2% (
0.1%) for the week to Sunday. These are on par with the seasonal average.- NSW: 2.3% (0.3%)
- VIC: 2.3% (0.2%)
- QLD: 2.2% (0.4%)
- SA: 2.3% (0.4%)
- WA: 1.9% (0.3%)
- TAS: 2.3% (0.3%)
- ACT: 1.4% (1.1%)
- NT: 0.5% (2%)

Flu Tracker is still showing a reduced level of general infections in those aged 16 years or older with at least three covid vaccinations. This is with only 4.2% of those aged 18-64 years having had a booster in the last 6 months.
Edit: Corrected the Flu Tracker estimate.
Yommie
SpeedLimited
- Oct 2, 2013
- 64,193
- 37,190
- Country of Origin
- Country of Residence
- Thread starter
- #985
COVID-19: Current cases – Health New Zealand | Te Whatu Ora
Read the latest information about confirmed and probable cases of COVID-19 in New Zealand.
 www.tewhatuora.govt.nz
www.tewhatuora.govt.nz
COVID-19: Current cases
Read the latest information about confirmed and probable cases of COVID-19 in New Zealand.This data is updated weekly. All data on this page relates to cases recorded prior to 11:59 pm 16 June 2024.
Whatu Tāniko pattern
On this page
- COVID-19 cases summary
- Current situation
- Deaths with COVID-19
- Case details
- Definitions
- Cases reported each day
- COVID-19 by location
- Total cases by location
This data is updated weekly. All data on this page relates to cases recorded prior to 11:59 pm 16 June 2024.
COVID-19 cases summary
| New case average* | RATs uploaded average* |
| 509 ↓ | 758 ↓ |
| Cases in hospital as at midnight Sunday | Cases in ICU as at midnight Sunday |
| 279 | 0 |
| Deaths attributed to COVID* | Total deaths attributed COVID |
| 5 ↑ | 4,120 |
Current situation
Summary| In the last week | New cases reported | 4788* |
|---|---|---|
| Reinfections | 3021 | |
| Reinfections (< 90 days) | 21 | |
| Total since first New Zealand case | Cases reported | 2663926 |
| Reinfections | 382057 | |
| Reinfections (< 90 days) | 26578 |
Case outcomes since first New Zealand case
| COVID-19 cases | Change in the last week | Total |
|---|---|---|
| Recovered | 4692 | 2656246 |
| Deceased* | 37 | 4120* |
Deaths with COVID-19
| Cause of death | Died within 28 days of positive test | Died more than 28 days after positive test | Total | Change in the last week |
|---|---|---|---|---|
| COVID as underlying | 2441 | 142 | 2583 | 23 |
| COVID as contributory | 1422 | 115 | 1537 | 14 |
| COVID-attributed total | 3863 | 257 | 4120 | 37 |
| Not COVID | 1907 | 0* | 1907 | 17 |
| Not available | 245 | 0 | 245 | -20 |
| Total | 6015 | 257 | 6272 | 34* |
Of the 34 people whose deaths we are reporting today: nine were from Auckland region, four were from Waikato, two were from Lakes, one was from Tairawhiti, one was from Taranaki, six were from Wellington region, two were from Nelson Marlborough, four were from Canterbury, one was from South Canterbury, four were from Southern.
One was in their 20s, two were in their 50s, three were in their 60s, nine were in their 70s, 15 were in their 80s and four were aged over 90. Of these people, 16 were women and 18 were men.
Case details
Number of active cases| Change in the last week | Total since first NZ case | |
|---|---|---|
| Confirmed | 3667 | 2618390 |
| Probable | -108 | 45536 |
| Total | 3559* | 2663926 |
Definitions
| Active case - confirmed | Confirmed cases are people who have received a positive PCR test OR someone who has received a positive result on a Rapid Antigen Test. For more details, see the COVID-19 case definition. |
|---|---|
| Active case - probable | A probable case is when someone is diagnosed based on their exposure to other people with COVID-19 and on their symptoms. |
| Reinfections | Reinfections are cases in an individual who reported a case 29 or more days previously. |
| Recovered | Recovered cases are people who had the virus, where at least 7 days have passed since their symptoms started and they have not had symptoms for 72 hours, and they have been cleared by the health professional responsible for their monitoring. |
| Deceased | Includes all deaths where COVID-19 is determined to have been the underlying cause of death or a contributory cause of death. |
Cases reported each day
Daily confirmed and probable cases

This graph shows the count of all cases of COVID-19 every day (all cases – confirmed and probable) since the first New Zealand case in late February 2020. The graph shows the rapid increase of daily cases from mid-February 2022 to early March 2022, driven by the Omicron variant.
From mid-March to mid-April 2022, cases rapidly declined, followed by a period of slower decline until early July. This was followed by a rapid increase in cases, peaking in August before a steady decline in new daily cases. Reported new daily cases hit their lowest since February 2022 in September 2022.
New COVID-19 cases reported each day
This graph shows the count of all cases of COVID-19 every day (all cases – confirmed and probable) since the first New Zealand case in late February 2020. The graph shows the rapid increase of daily cases from mid-February 2022 to early March 2022, driven by the Omicron variant.
From mid-March to mid-April 2022, cases rapidly declined, followed by a period of slower decline until early July. This was followed by a rapid increase in cases, peaking in August before a steady decline in new daily cases. Reported new daily cases hit their lowest since February 2022 in September 2022.
COVID-19 by location
Total cases by location

This bar graph shows the total cases and their status by health district and those with recent travel history.
The ‘At the border’ data group includes cases detected in managed isolation or quarantine facilities from the period when these were operating, as well as cases with recent travel history from after that time. They are not included in the district totals. Before 17 June, people in managed isolation or quarantine facilities were included in the total of the relevant district.
Total COVID-19 cases by location graph
This bar graph shows the total cases and their status by health district and those with recent travel history.
The ‘At the border’ data group includes cases detected in managed isolation or quarantine facilities from the period when these were operating, as well as cases with recent travel history from after that time. They are not included in the district totals. Before 17 June, people in managed isolation or quarantine facilities were included in the total of the relevant district.
Total cases by location
| Location | Active | Recovered | Deceased | Total | New cases in the last week |
|---|---|---|---|---|---|
| Auckland | 339 | 249801 | 280 | 250420 | 458 |
| Bay of Plenty | 135 | 116760 | 195 | 117090 | 181 |
| Canterbury | 567 | 352342 | 560 | 353469 | 763 |
| Capital and Coast | 353 | 189368 | 190 | 189911 | 444 |
| Counties Manukau | 296 | 296430 | 329 | 297055 | 384 |
| Hawke's Bay | 113 | 87263 | 174 | 87550 | 151 |
| Hutt Valley | 218 | 92629 | 100 | 92947 | 302 |
| Lakes | 58 | 51950 | 113 | 52121 | 76 |
| Mid Central | 105 | 98534 | 214 | 98853 | 137 |
| Nelson Marlborough | 146 | 81287 | 168 | 81601 | 184 |
| Northland | 79 | 82462 | 155 | 82696 | 111 |
| South Canterbury | 66 | 35208 | 47 | 35321 | 90 |
| Southern | 304 | 194929 | 393 | 195626 | 406 |
| Tairāwhiti | 43 | 27047 | 46 | 27136 | 63 |
| Taranaki | 59 | 66703 | 132 | 66894 | 79 |
| Unknown | 0 | 2301 | 9 | 2310 | NA |
| Waikato | 241 | 211892 | 420 | 212553 | 351 |
| Wairarapa | 27 | 26146 | 68 | 26241 | 35 |
| Waitematā | 359 | 314613 | 420 | 315392 | 497 |
| West Coast | 8 | 16040 | 22 | 16070 | 10 |
| Whanganui | 44 | 35249 | 79 | 35372 | 66 |
| At the Border* | 0 | 27292 | 6 | 27298 | NA |
| Total | 3560 | 2656246 | 4120 | 2663926 | 4788 |
You can also view a detailed breakdown of daily case numbers for each district since the beginning of the pandemic by clicking the ‘download’ button on the right hand side of this page: New Zealand COVID-19 data.
Note: we cannot give detailed information about cases in your district, city or town, as we must protect the privacy of the people concerned.
Also in this section
Last updated: 17 June 2024Yommie
SpeedLimited
- Oct 2, 2013
- 64,193
- 37,190
- Country of Origin
- Country of Residence
- Thread starter
- #986

Quick update on Covid in England. Plus manifestos!
Modest May wave over, but likely to be another wave this month. Plus a quick look at the party manifestos.
Quick update on Covid in England. Plus manifestos!
Modest May wave over, but likely to be another wave this month. Plus a quick look at the party manifestos.

CHRISTINA PAGEL
JUN 13, 2024
52
7
Share
What happened in May?
The monthly update of hospital admissions with Covid has been published by NHS England today. It shows the clear wave in May, but also shows that it was smaller than the autumn and winter waves. [Note: yes hospitals are testing less than they were, but their testing protocols have been pretty constant over the last year].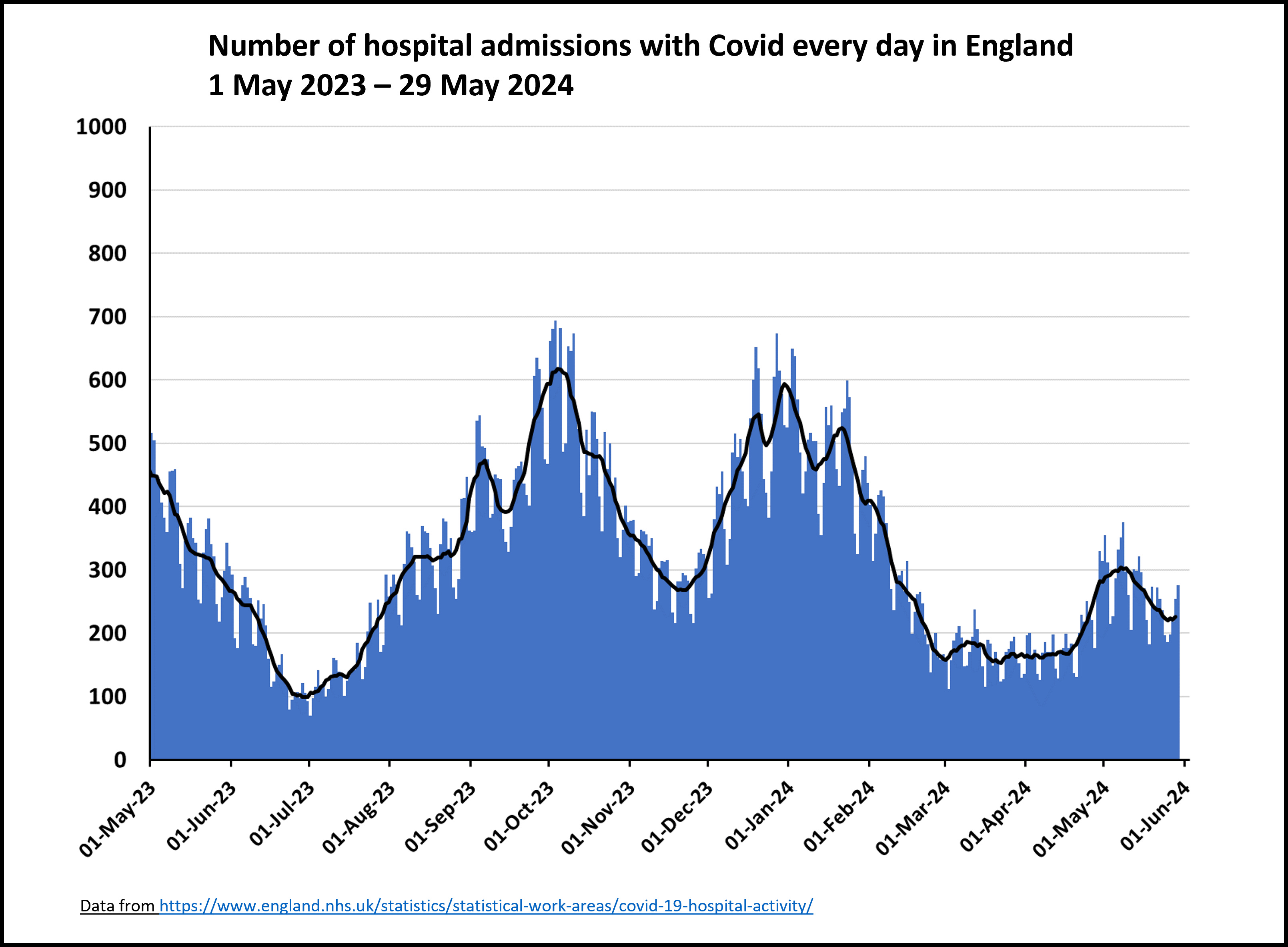
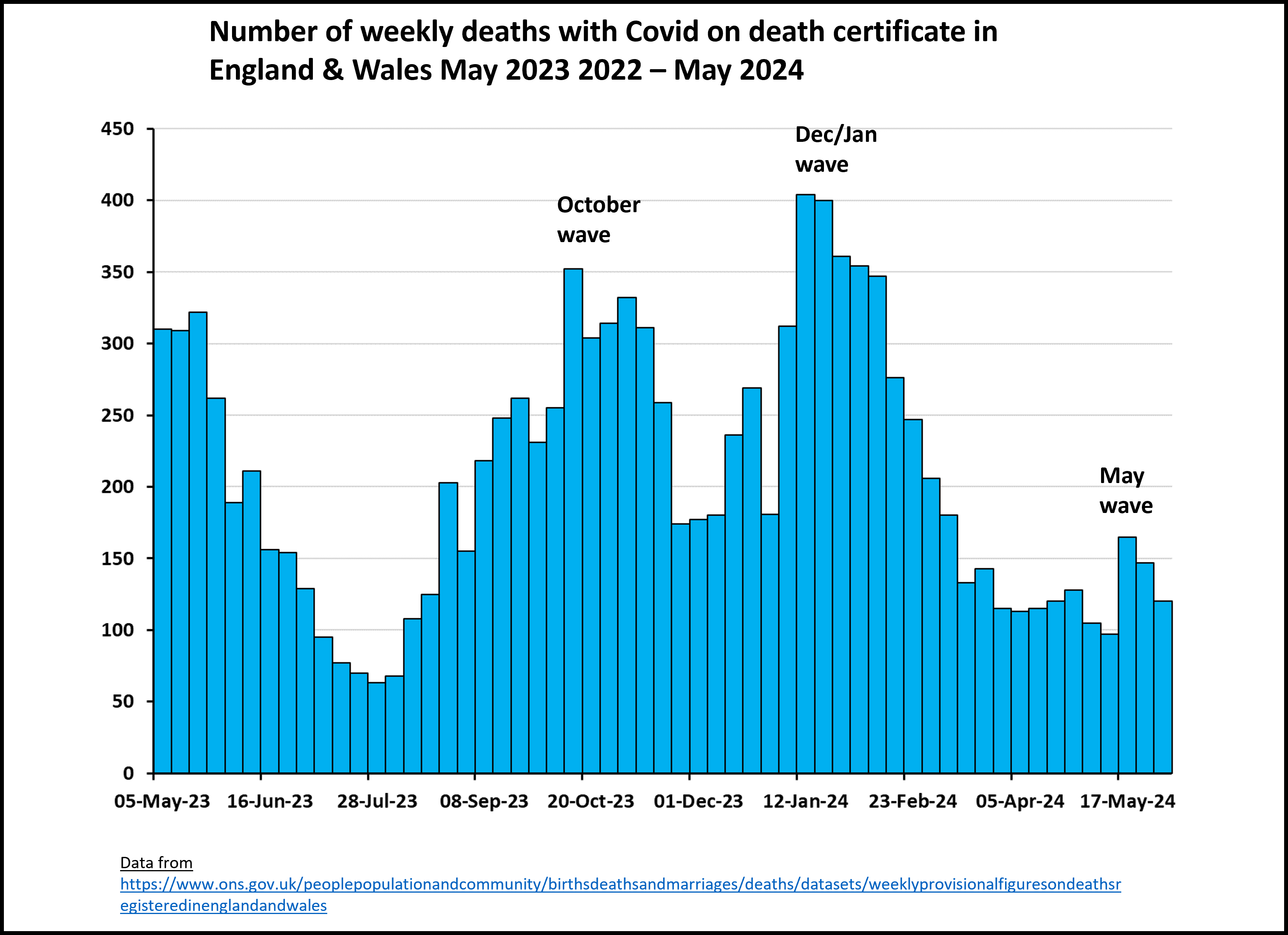
The May wave was likely driven by a combination of waning immunity and the growth of the KP.2 coronavirus variant (a child of JN.1 which caused the Christmas 2023 wave). The wave is also visible in weekly registered deaths, but again the number of deaths were much lower than the previous two waves.
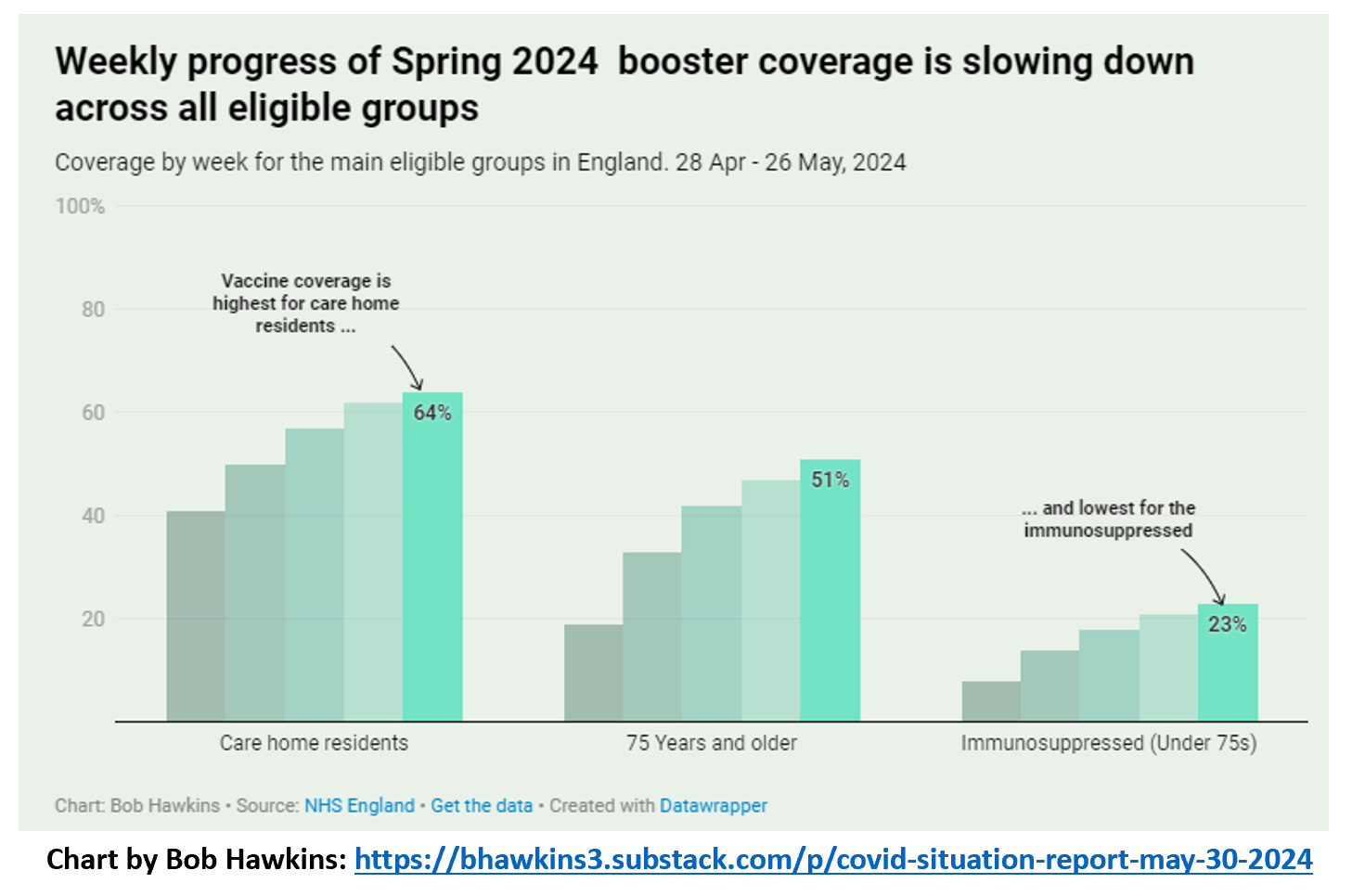
Covid’s impact will have been (thankfully) blunted by many of the most vulnerable receiving a Spring Vaccine Booster, particularly those in care homes, although coverage in the immunosuppressed remains worryingly low.
Subscribe
What’s next?
However, there are hints in the most recent data to end of May that admissions may be rising again. We also know that the KP.3 subvariant (a more rapidly spreading sister to KP.2) is growing in the UK (estimated at about 30% of sequenced tests by the end of May). I don’t know whether the KP.3 wave will be bigger than the KP.2 May wave, but I am pretty sure that it will cause another wave making this summer a more Covid-prevalent summer than last year where June and July were very quiet months.That said, we can perhaps look to countries ahead of us on the KP.3 curve for clues. One of these is Portugal where about two thirds of their sequenced cases are KP.3 and they are experiencing a surge in both cases and hospitalisations.

Another example is California where KP.3 is dominant and which is currently seeing a surge in wastewater detected Coronavirus and in hospitalisations.
We sadly (and shamefully) do not have wastewater monitoring in England. However Scotland wastewater monitoring shows (modest) increases to the 6 June, which are also reflected in Scottish hospital admissions. Eslewhere in Europe, Belgium and Denmark are seeing definite increases in wastewater signals but the picture is more mixed elsewhere.

My overall feeling is that we should definitely expect a June covid wave, bigger than May but hopefully not as big as the JN.1 winter wave. And as ever, it’s not just the impact on acute illness that matters, but also Long Covid (e.g. my substack from April). There is still far too little available in the way of treatment, and each new wave leads to more people living with this potentially debilitating condition.
Please do accept any booster offer you are offered - even if the Covid boosters are based on variants that do not precisely match the current circulating variants, they still provide a great deal more protection than not getting vaccinated at all!
Prof Sheena Cruickshank also offers an update on future Covid-19 vaccines in her recent substack.
Share
Manifesto!
This week has seen the release of the UK party manifestos. It was really encouraging to see both the Greens and the Liberal Democrats commit to implementing a Clean Air Act. The Liberal Democrats go further and also commit to implementing “a post-pandemic strategy for supporting people who are immunocompromised” and learning more broadly from the country’s experiences of the pandemic.https://substackcdn.com/image/fetch...518-12c7-401d-88fe-57f417544273_2996x1407.png
Labour’s manifesto does not mention indoor air quality or cleaner air, but it does commit to implementing the findings from the Covid-19 Inquiry - which could include such measures and hopefully a whole host of other measures designed to improve the country’s resilience to future pandemics.
https://substackcdn.com/image/fetch...c68ac-172d-41f9-ad47-9e791ca44112_746x336.png
The Conservatives mention neither indoor air quality nor the Covid-19 Inquiry. Instead, they praise their pandemic record (!) and commit to supporting the NHS recovery. They do however discuss developing a National Defence and Resilience Plan which includes pandemics in its remit and to use “learnings from Covid to improve the country’s preparedness for risks on the National Risk Register”.
So from a purely Covid-19 perspective (and thinking also about the potential for avian flu (H5N1) to cause a devastating pandemic relatively soon!), there are some things to celebrate in the Liberal Democrat and Green Party manifestos. Labour says little about it but if it actually did implement the findings of the Covid-19 Inquiry in full, that would be a substantial improvement. The Conservatives don’t commit to anything specific and so it is difficult to say much positive about their plans in respect of Covid-19 or future pandemics.
Yommie
SpeedLimited
- Oct 2, 2013
- 64,193
- 37,190
- Country of Origin
- Country of Residence
- Thread starter
- #987

The Covid Conspiracy
Deceptive scientists have been trying to prevent a legitimate investigation into how the Covid-19 pandemic began. That anti-science conspiracy is an extremely insidious threat to all of our safety.
The Covid Conspiracy
Deceptive scientists have been trying to prevent a legitimate investigation into how the Covid-19 pandemic began. That anti-science conspiracy is an extremely insidious threat to all of our safety.

WILLIAM SANCHEZ
JUN 15, 2024
2
Share
The origin of Covid is one of the most interesting stories in recent scientific history. Millions of people around the world died as a result of the pandemic and society came to a grinding halt. Any reasonable person would want to figure out how that pandemic started to prevent that same situation from happening again. This is a matter of extreme public importance in which discovering the truth about how Covid-19 started has the potential to help prevent future pandemics and save millions of lives. There are two main pathways that could have created the virus which started the pandemic; natural evolution or a research-related incident. Unfortunately when it comes to the possibility that Covid-19 could have resulted from a research-related incident, many disingenuous scientists would prefer if we never discovered the origin. There is an anti-science conspiracy going on which aims to downplay & stigmatize the lab leak hypothesis while slandering any scientist investigating that pathway. That anti-science conspiracy greatly exaggerates evidence supporting a natural origin of the virus while simultaneously ignoring or diminishing evidence supporting a hypothesized lab leak. Fake news is created by deceptive scientists and science journalists to misinform their audience regarding the actual evidence while deceitfully describing the legitimate origin investigation as anti-science. Disappointingly, the lab leak investigation has been consistently obstructed by that anti-science conspiracy, costing the world years of delayed investigations.
The reality is, after an extensive search for the natural origin of the virus, none has been found. In response to claims the the Huanan Seafood Market sparked the outbreak, Senator Richard Burr noted that after extensive testing, “none of the animals at the market when it was closed, in the market’s supply chain, or in China’s animal farming industry were infected with SARS-CoV-2. That would be a significant variation from multiple precedents from previous natural zoonotic spillovers” (HELP, pg. 10). According to the Lancet’s Covid Commission, "Despite the testing of more than 80,000 samples from a range of wild and farm animal species in China collected between 2015 and March, 2020, no cases of SARS-CoV-2 infection have been identified" (Lancet). So, after a years-long search for the hypothesized animal reservoir, including testing more than 80,000 animal-related samples, no host species for the virus has been identified. The natural evolution hypothesis is weakly supported by;
- an epidemiological analysis of the known early cases looking at their proximity and relation to the Huanan Seafood Market,
- the identification of animal DNA from species hypothesized to be a likely animal reservoir alongside the virus found in swabs from within the Huanan Seafood Market taken in January 2020,
- and the identification of 2 strains of the virus in the HSM, also when it was tested in January.
- the early case definition was “an unknown virus linked to the market,” so analyzing early case data which only includes known cases collected with that bias will inevitably show biased results,
- some susceptible animals were kept at the HSM, but that does not mean they were the source of the pandemic. Weeks into the outbreak when environmental samples were collected, people would’ve already taken the virus into the market. Animals tested from the HSM supply chain, other markets in Wuhan, and samples from within the HSM failed to locate a natural reservoir of the virus.
- and weeks into the pandemic both strains were likely taken into the HSM through humans with the HSM acting as an early super-spreader event, not the source.
We know that;
- researchers at the WIV collected thousands of natural bat viruses from remote locations making the WIV one of the largest repositories of those viruses in the world; many of those viruses remain undisclosed,
- researchers at the WIV created coronavirus chimeras, performed transgenic mouse model experiments, and “left no traces of genetic modification of SARS-like coronaviruses” (ODNI),
- researchers at the WIV, in collaboration with US scientists, proposed to locate a highly infectious SARS virus or create one in the lab if one could not be located,
- researchers at the WIV worked in BSL-2 conditions and had covid-19-like symptoms right before the pandemic began,
- the reported names of the 1st three people to ever have Covid-19 from the WIV were leaked to two different journalists each citing multiple current and former US government officials as their sources,
- & that the evidence behind those leaked reports of patient 0 was ordered to be disclosed by the Intelligence Community in the Covid Origins Act of 2023, but that evidence is being illegally withheld by the Director of National Intelligence still to this day.
In January 2021 a US State Department Fact Sheet made some serious accusations;
- “The U.S. government has reason to believe that several researchers inside the WIV became sick in autumn 2019, before the first identified case of the outbreak, with symptoms consistent with both COVID-19 and common seasonal illnesses…
- The WIV has a published record of conducting “gain-of-function” research to engineer chimeric viruses. But the WIV has not been transparent or consistent about its record of studying viruses most similar to the COVID-19 virus…
- the United States has determined that the WIV has collaborated on publications and secret projects with China’s military. The WIV has engaged in classified research, including laboratory animal experiments, on behalf of the Chinese military since at least 2017.” -US State Department
Former Director of National Intelligence John Ratcliffe had seen that evidence for himself. Based on his judgement of that evidence, he said; "My informed assessment as a person with as much access to intelligence as anyone in the initial year of the pandemic...is that a lab leak is the only explanation credibly supported by our intelligence, the science, and common sense" (Ratcliffe). He then advocated for that evidence to be made public in compliance with the Covid Origin Act of 2023;
So we have the former Director of National Intelligence asserting that a lab leak is the only explanation credibly supported by US classified intelligence. We have a former State Department official claiming classified evidence of patient 0 is the best indication of how the pandemic started. Leaks to journalists have exposed the names of the 1st three ever cases of Covid-19 from the WIV based on multiple current and former US government officials. We are possibly just 1 step away from total confirmation of a lab leak origin of the Covid-19 pandemic and that fact should be the single biggest focus of the origin investigation. The best way to further the investigation is for the United States Congress to hold a hearing with subpoenas for the DNI plus heads of the FBI, CIA, & DoE to ask them every question of the Covid Origins Act under oath in public. Actually, Section 3 part C #1-7 are the most important part to ask the DNI;
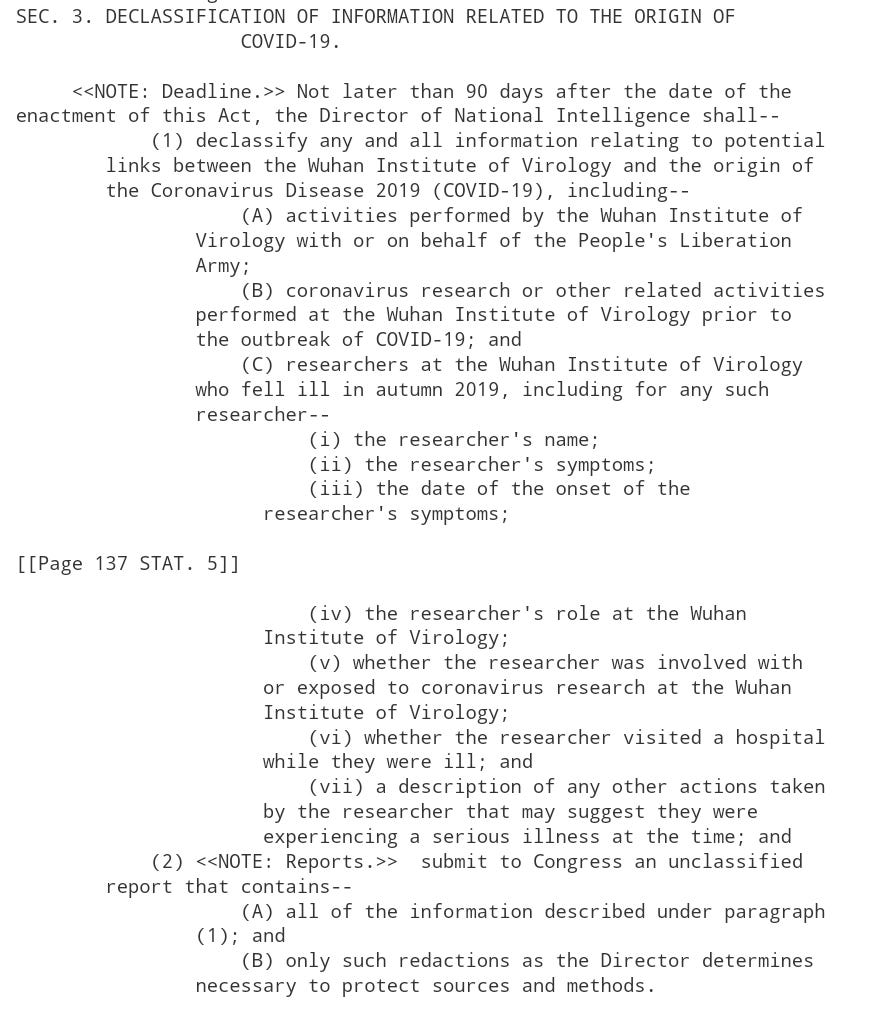
Covid Origins Act
So that’s where the 2 origin investigations are at. At this point a lab leak is significantly more likely as an origin of the Covid-19 pandemic based on the available evidence. If the pandemic really began through a lab leak, and that research is continuing in unsafe conditions, then millions of people are at risk from future man-made pandemics. How Covid-19 actually began is too important an issue for the world to leave unsolved when the truth is within reach! We need to get the truth out into the open and strictly regulate the dangerous research which likely caused the Covid-19 pandemic. Alina Chan has been an exceptional scientist truly standing up for the "integrity of science itself" as the Lancet Covid Commission encouraged. She wrote an excellent NYT opinion piece explaining the evidence supporting a research-related origin of the Covid-19 pandemic. More importantly, she encouraged much needed regulation and oversight of the dangerous research which likely caused the pandemic;
"A successful investigation of the pandemic’s root cause would have the power to break a decades-long scientific impasse on pathogen research safety, determining how governments will spend billions of dollars to prevent future pandemics. A credible investigation would also deter future acts of negligence and deceit by demonstrating that it is indeed possible to be held accountable for causing a viral pandemic. Last but not least, people of all nations need to see their leaders — and especially, their scientists — heading the charge to find out what caused this world-shaking event. Restoring public trust in science and government leadership requires it.
A thorough investigation by the U.S. government could unearth more evidence while spurring whistleblowers to find their courage and seek their moment of opportunity. It would also show the world that U.S. leaders and scientists are not afraid of what the truth behind the pandemic may be." -Alina Chan
The best way to push back on the false narrative created by deceptive scientists engaged in an anti-science conspiracy is to get the truth out there. In order to offset that anti-science conspiracy, I’ve written these papers to tell the real story;
Why is there an Investigation into the Origins of Covid-19?
The Science of the Lab Leak Theory
Why Prosecute/Fauci?
Failure to Comply
Where is the Covid-19 Origins Investigation Now?
and I recorded this podcast The Origin of Covid-19
Subscribe
Share
The need for an honest investigation into the origin of Covid-19 has been the scientific consensus since 2022. Any source that has claimed differently since then should be met with the utmost skepticism. This post of mine on Twitter/X from November 2022 quotes the final report from Lancet Medical Journal’s Covid Commission;
The Lancet Covid Commission represents the real science on the topic.
Follow the Science!
Yommie
SpeedLimited
- Oct 2, 2013
- 64,193
- 37,190
- Country of Origin
- Country of Residence
- Thread starter
- #988

Summer COVID surge approaches in Seattle area as travel season begins
A summer COVID-19 surge is making its way through the region. It's time to mask up while traveling and take extra precautions, public health officials say.
 www.seattletimes.com
www.seattletimes.com
Summer COVID surge approaches in Seattle area as travel season begins
June 17, 2024 at 6:00 am Updated June 17, 2024 at 6:00 am")
Passengers wearing masks walk with luggage near an Alaska Airlines check-in area at Seattle-Tacoma International Airport in Seattle. (Ted S. Warren / The Associated Press, 2021)
Skip Ad

By
Elise Takahama
Seattle Times staff reporter
A summer COVID-19 surge is on its way through Seattle and the region.
Infection rates and emergency department visits in King County have been rising since the end of April, causing some concern among doctors and public health officials as travel season picks up and people begin gathering more frequently.
“This is the time when people should start taking precautions,” said Dr. Eric Chow, King County’s chief of communicable diseases. “I don’t know how high this [peak] is going to be, when it’s going to peak, but taking precautions now is the best way for people to be able to mitigate the complications related to COVID.”
King County’s virus-related emergency department visits hit a new low the week ending April 27, when only about 0.5% of visits involved a COVID diagnosis. As of last week, COVID patients made up about 1.5% of hospital emergency visits.
More on COVID-19
- Seattle’s summer COVID surge is here; what to know
- Another COVID vaccine? Yes, and here’s why
- A guide to managing COVID this summer
- New report underscores the seriousness and extent of long COVID
- Four years on, COVID-19 remains a worse killer than the flu
- Your 2024 guide to COVID symptoms and treatment
- Our collected list of stories about COVID-19
ADVERTISING
Skip Ad
Skip Ad
Skip Ad
But because fewer people are testing themselves for COVID and emergency department data generally lags behind waves of infection, Chow noted there’s “probably a lot more community transmission that’s happening that’s not fully captured in the data here.”
State COVID emergency department visits have also gradually increased since the end of April, though at a slightly slower rate — jumping from about 0.5% to 1% of total emergency department visits. Statewide death rates have remained low for months, though more than 400 people in Washington have died from the virus since January.
Infectious-disease experts in Seattle and other parts of the country are also keeping an eye on the ever-growing list of variants that continue to battle for dominance and drive bumps in cases and hospitalizations.
In Washington, omicron subvariant JN.1, the winter’s dominant strain, is still the most common, responsible for about 40% of cases. Other omicron subvariants, including JN.1.11.1, JN.1.7 and KP.1.1, each make up about 20% of cases here, according to the state Department of Health’s respiratory disease dashboard.
Nationally, KP.2 and KP.3 have also begun to make up a greater proportion of infections, according to the Centers for Disease Control and Prevention.
The virus’s ability to mutate and evolve remains strong, which is why public health officials are again urging people to stay up to date with COVID vaccinations.
ADVERTISING
Skip Ad
Skip Ad
Skip Ad
“COVID is behaving just as it has throughout the pandemic,” Chow said. That means, he said, “more variants [are] trying to evolve and find ways to evade our existing immunity.”
Vaccination rates, federal funding drops
In King County, vaccination rates have fallen since last October, after the most recently updated shot became available. Statewide, just 19% of Washingtonians are up to date with their COVID vaccinations, although nearly 70% have been vaccinated with their full primary series.Chow expressed disappointment in decreases in federal funding since the height of the pandemic and acknowledged his department doesn’t have the same capacity it once did to ensure comprehensive access to vaccines and testing. Public Health – Seattle & King County’s longtime mass COVID vaccination clinic in Kent and drive-thru site at Snoqualmie Valley Hospital, for example, both closed at the end of March.
“With the available resources we have, including some limited vaccine clinics, we’ve tried to focus on communities who have the least amount of access, trying to bridge that gap,” Chow said. “But it is a huge concern of mine.”
The health department noted many community health centers, most pharmacies and other health care providers can still offer COVID vaccinations. More information about where to find a site is available at vaccines.gov.
The CDC recommends an updated vaccine shot for everyone 6 months and older. Those 65 and older should get two shots, as long as four months have passed since their first, according to the CDC.
ADVERTISING
Skip Ad
Another update on COVID vaccines will likely come later this year, as scientists tackle ways to keep Americans safe during the upcoming season. The newest shot, recommended by the FDA last week, will target a variant of JN.1.
But before those shots become available, public health officials are pushing people to get the most updated immunizations already on the market. Take those precautions before heading off on vacation, and consider wearing a mask while in airports or on planes, Chow said.
For those at high risk of severe infection, he also recommended checking in with a health care provider about ways to stay safe while traveling. He urged COVID patients eligible for an antiviral treatment to seek that option early in their diagnosis to help protect them from hospitalization or death.
“We’re excited that people now have the ability to travel,” he said. “But this poses a new risk that we didn’t see at the same degree during the height of the pandemic.”
Users who are viewing this thread
Total: 1 (members: 0, guests: 1)
Pakistan Defence Latest
-
Durga Puja gift: Bangladesh interim government to export 3,000 tonnes of hilsa to Bengal (4 Viewers)
- Latest: Vikramaditya1
-

-

-

Country Watch Latest
Latest Posts
-
-
-
Xi Jinping Triggers Outrage! Despite China’s Economic Hardships, Gifts $50 Billion to Africa. (10 Viewers)
- Latest: liuzhengdong
-

-