Yommie
Elite Member
- Oct 2, 2013
- 64,101
- 37,185
- Country of Origin

- Country of Residence

- Thread starter
- #2,161

COVID activity is high, but Canada not 'remotely close' to worst days of the pandemic: experts
The COVID surge is being driven by highly contagious Omicron offshoots, sub-variants from the JN.1 lineage that drove last winter's spike
 nationalpost.com
nationalpost.com
COVID activity is high, but Canada not 'remotely close' to worst days of the pandemic: experts
The latest COVID surge is being driven by highly contagious Omicron offshoots, sub-variants from the JN.1 lineage that drove last winter's spikeGet the latest from Sharon Kirkey straight to your inboxSign Up
Author of the article:
Sharon Kirkey
Published Sep 05, 2024 • Last updated 1 hour ago • 6 minute read
214 Comments

Article content
Nearly five years into its emergence in humans, wastewater data suggest SARS-CoV-2 activity is high across most of Canada, driven by variants that are significantly different from strains circulating even a year ago.Weekly deaths, however, remain low overall — 54 deaths were reported nationally the week ending Aug. 24 — and nowhere near peak pandemic levels, according to the federal government’s most recent COVID epidemiology update. More than 900 deaths were reported in the third week of January 2022, the deadliest week on record, during the early Omicron surges.
Advertisement 2
Story continues below
“We’re not seeing waves of people ending up in hospital like we did earlier in the pandemic,” said Dr. Fahad Razak, an internist at St. Michael’s Hospital in Toronto.
“That’s a good thing. That should be celebrated. That reflects the broad immunity in the population,” Razak said.
Still, “in my hospital and hospitals across the province” people with COVID are ending up in hospital, though far fewer than before, infections can be unpredictable even in healthy people and long COVID remains an issue, Razak said. SARS-CoV-2 is also mutating, rapidly, to shake off immunity from previous vaccinations and infections and reinfect people.
Article content
“I don’t think the majority of scientists who were looking at this early in 2020 or at the end of 2019 expected that, four years later, we’d be dealing with unrelenting waves of variants, which are immune evasive,” Razak said.
“We haven’t seen a widely distributed virus in recent human history that has had this property.”
That pattern of rapid mutation is the norm, making it all the more important to get updated vaccines to the highest risk groups, he and others said. But it could be another month before Health Canada approves three reformulated vaccines — and there’s confusion over whether the old formulas will be available until then.
Advertisement 3
Story continues below
Article content
Ontario and several other provinces issued notices that Health Canada had ordered remaining supplies of last spring’s booster shots targeting the then-dominant XBB strain quarantined and destroyed effective Sept. 1 to make way for the new updated vaccines, creating a gap where no vaccine would be available.
“If you want a vaccine in September, forget about it,” University of Ottawa’s Amir Attaran said on X, formerly Twitter.
“It doesn’t make any sense to me — the obviously reasonable thing to do is get your new vaccine in hand, before withdrawing the old one,” Attaran, a professor in the faculty of law and School of Epidemiology, Public Health and Community Medicine, told National Post.
“You don’t strip yourself naked when your clothes are in the washing machine.”
The old vaccines are still modestly effective, he said. “Why destroy vaccines during a big COVID wave?”
In a statement to National Post, the Public Health Agency of Canada (PHAC) said withdrawing existing XBB vaccines “is part of regulatory and supply management best practices,” consistent with the approach to annual flu shots.
NP Posted
Get a dash of perspective along with the trending news of the day in a very readable format.
Sign Up
By signing up you consent to receive the above newsletter from Postmedia Network Inc.
Article content
Advertisement 4
Story continues below
Article content
A transition plan to move from the current supply to updated vaccines targeting current strains “provides each province and territory the flexibility to ensure ongoing access to current supply until new vaccines are approved,” the agency said. “This includes a period of transition to full removal.”
The government also maintains a federal reserve of XBB vaccines “for any unexpected public health need,” the statement said.
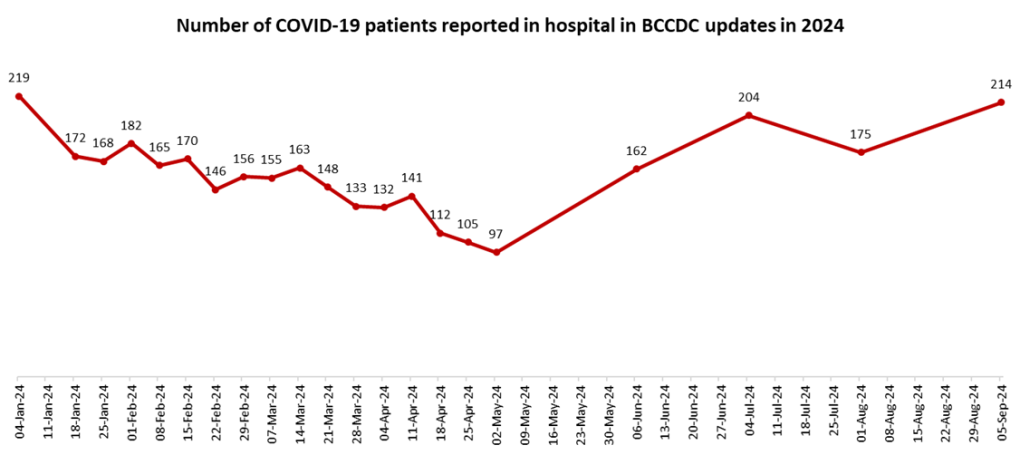
COVID outbreaks in long-term care and other congregate settings have been slowly increasing since June. Concentrations of virus detected in wastewater — sewage — indicates “high” levels of COVID activity in British Columbia, Manitoba, Ontario, Nova Scotia and Newfoundland and Labrador, and “moderate” activity in the Yukon, Quebec, Prince Edward island and New Brunswick, according to a federal wastewater monitoring dashboard that covers just 29 per cent of the population.
With schools reopened and flu and other seasonal respiratory viruses on the doorstep, “we’re trending towards a not-so-good place right now,” said Dr. Nitin Mohan, an assistant professor at Western University’s Schulich School of Medicine and Dentistry.
Advertisement 5
Story continues below
Article content
We clearly have no reliable ability to predict the evolutionary trajectory of the virus
The latest COVID surge is being driven by highly contagious Omicron offshoots, sub-variants from the JN.1 lineage that drove last winter’s spike.
Health Canada is reviewing Pfizer and Moderna’s formulations targeting KP.2, and Novavax’s against JN.1, although another sub-variant, KP.3.11 now accounts for more than half of sequences tested, and growing.
The only thing a virus “cares” about is its ability to spread, said Matthew Miller, Canada Research Chair in viral pandemics at McMaster University.
Today’s sub-variants, dubbed FLiRT for their mutations, have made a pair of mutations that help the virus dodge antibodies produced by previous infections and vaccinations and evade pre-existing immunity — mutations that on their own make the virus less able to stick to our cells and infect us.
To compensate, the variants have made mutations in a different part of the virus that make it better able to bind to and infect cells.
A remarkable mutation event like the emergence of Omicron, which had more than 50 known mutations compared to Alpha, Delta and earlier strains, is unlikely.
Advertisement 6
Story continues below
Article content
But almost every three to four months, the virus becomes different enough “that a large group of the population no longer has sufficient immunity to prevent infection,” Miller said.
It’s proving hard to keep up. “We clearly have no reliable ability to predict the evolutionary trajectory of the virus,” Miller said. “We just don’t have the models that tell us, ‘How is this virus going to change in three months so that we can make a vaccine that will reflect the new virus that doesn’t exist yet?'”
Even when mismatched, the vaccines tend to do an “exceptionally good job.” The protection from infection is relatively short-term, but protection against severe disease lasts longer. “Their ability to protect against severe infections, hospitalization and death remain stable over much longer periods.”
“I think we should expect the same thing from these upcoming vaccines,” Miller said.
Unlike influenza or respiratory syncytial virus, COVID is very much a year-round virus and tends to peak every three to six months, though “there really isn’t a time when the virus is non-existent,” Mohan said. “We’re still seeing deaths from SARS-CoV-2 in numbers that people from my world feel are significantly higher than they should be.”
Advertisement 7
Story continues below
Article content
Those most at risk of severe COVID include people over 65, people with heart disease, diabetes, cancer or other underlying medical conditions, people who take immunosuppressive drugs, pregnant women and children with complex medical needs.
Cold and flu-like symptoms continue to be the main symptoms, but there’s lots of variability, Miller said.
“We should respect that the viral evolution has been highly unpredictable,” said Razak, a Canada Research Chair at the University of Toronto.
“In a year or two years, maybe we’re presented with a different situation. But based on today’s variant, the pattern of illness, the pattern of severe illness, there is nothing to suggest that we’re anywhere close — remotely close — to what we experienced even a couple of years ago.”
Alberta saw 25 per cent fewer COVID-related deaths in the last season (which ended Aug. 24) compared to the previous season, the Edmonton Journal reported.
However, Quebec saw higher mortality rates during this summer’s COVID wave than last year’s, the Montreal Gazette reported.
“We should, in general, try to prevent infections where possible, and, for the highest risk people, we need to get (the newer) vaccine, ideally timed to prevent critical illness like hospitalization,” Razak said.
Advertisement 8
Story continues below
Article content
But COVID isn’t the only virus spreading. Many parts of the country are seeing higher rates of pertussis, or whooping cough, and while waiting for the updated vaccines there’s a “whole portfolio” of other strategies to reduce the spread of respiratory viruses in general, Razak said, including opening windows to improve ventilation, not exposing others when you’re sick and masks for high-risk people in high-risk settings.
Only about half of people in higher risk age groups were vaccinated with the updated XBB booster shots in the spring campaigns. “There’s an opportunity to protect people most at risk,” Razak said. “When the (new) vaccines become available, those vaccine rates should be higher than what we saw in the spring.”