Navigation
Install the app
How to install the app on iOS
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
More options
Style variation
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Covid-19 News and Discussions
- Thread starter Yommie
- Start date
Yommie
SpeedLimited
- Oct 2, 2013
- 64,204
- 37,191
- Country of Origin

- Country of Residence

- Thread starter
- #497

3 more COVID deaths in New Brunswick, 4 youth among flu hospitalizations
Three more New Brunswickers have died from COVID-19, while no new influenza deaths have been reported, and hospitalizations for both viruses have decreased, updated data from the province Tuesday shows.A child under four, and three youth aged five to 19 are among those hospitalized by the flu...
3 more COVID deaths in New Brunswick, 4 youth among flu hospitalizations
CBC
Tue, March 26, 2024 at 12:38 p.m. EDT·4 min read
")
Since the beginning of the respiratory season on Aug. 27, 86 New Brunswickers have died from COVID, there have been 1,396 hospitalizations and 91 intensive care admissions. (CBC - image credit)
Three more New Brunswickers have died from COVID-19, while no new influenza deaths have been reported, and hospitalizations for both viruses have decreased, updated data from the province Tuesday shows.
A child under four, and three youth aged five to 19 are among those hospitalized by the flu between March 10 and March 16, according to the Respiratory Watch report.
"COVID-19 activity remains moderate; some indicators (number of cases, percent positivity, and hospitalizations) decreased slightly during the current reporting period," it says.
Influenza activity "slightly decreased" during the reporting week.
Of the three people who died, one was aged 45 to 64 and the other two were aged 65 or older.
Their deaths raise the province's pandemic death toll to at least 1,022. The actual total is unclear because the Department of Health counts only people who die in hospital as COVID deaths.
Fifteen people were hospitalized because of COVID or for something else and later tested positive, down from 21 in the previous report.
One person required intensive care, unchanged.
Of those hospitalized, three are aged 45 to 64, and 12 are aged 65 or older, including the one in ICU.
6 outbreaks, 40 new cases
Six lab-confirmed COVID outbreaks have been declared, the same number as the previous week. Four are in nursing homes and two are in facilities described only as "other."
Forty new cases of COVID have been confirmed through PCR (polymerase chain reaction) lab tests, down from 60.
The positivity rate — or the percentage of lab tests performed that produced a positive result — is three per cent, down from five.
428 more vaccines administered
About 400 New Brunswickers rolled up their sleeves to get a COVID-19 vaccine in the past week, after the Department of Health urged anyone who has not received a vaccine or had a COVID infection within the last six months to get a shot soon to ensure they are protected and to ensure they meet the recommended six-month interval to get a fall vaccine.
A total of 147,677 XBB.1.5 vaccines have been administered since Oct. 4, figures from the department show.
Spring COVID-19 vaccine boosters will be available April 2 through June 15 for New Brunswickers considered most at risk of severe illness, the department announced last week. This includes people aged 65 or older, residents of nursing homes and adult residential facilities and immunocompromised people aged six months or older.
. September, 2023.")
Comirnaty, the Pfizer-BioNTech COVID-19 vaccine (booster). September, 2023.
Although spring boosters won't be administered until April 2, bookings for appointments opened up on Monday. (Joe Burbank/The Associated Press)
Eligible New Brunswickers can book appointments now, either online, by calling 1-833-437-1424 or by contacting a participating pharmacy.
People who do not meet the eligibility guidelines but received a fall or winter dose as part of the current vaccination campaign, which began Oct. 16, "are considered fully up to date, and do not require another vaccine this spring," department spokesperson Sean Hatchard said.
Flu sends 13 to hospital, 2 to ICU
The flu sent 13 people to hospital between March 10 and March 15, down from 23 in the previous report.
Two of them required intensive care, up from none.
In addition to the four youth hospitalized, there were also two people aged 20 to 44, and seven people aged 65 or older, including the two in ICU, the report shows.

A hospital room with a vacant bed.
The flu has hospitalized 506 people since the respiratory season began on Aug. 27, 47 of whom required intensive care, according to the Respiratory Watch report. (CBC)
Ninety-nine new cases of the flu were confirmed through lab tests, down from 145, and the positivity rate is nine per cent, down from 12.
The breakdown of new cases includes 64 influenza B and 35 influenza A.
There have now been 2,998 cases reported since the respiratory season began on Aug. 27
Three lab-confirmed influenza outbreaks have been declared — one in a nursing home and two in "other facilities." A week ago, none were reported.
There was also one "influenza-like illness" outbreak reported at a school, up from none. No other details are provided, but school outbreaks are based on 10 per cent absenteeism because of influenza-like illness symptoms, according to the report.
As of Tuesday, a total of 222,394 New Brunswickers have been vaccinated against the flu this season, up from 221,808 a week ago, the Department of Health said.
Vitalité releases monthly COVID update
Vitalité Health Network posted its monthly COVID-19 update Tuesday. It shows 15 COVID-positive health-care workers are off sick, as of Saturday, down from 33 in the February report.
There are six hospitalized COVID patients, up from five. None require intensive care, unchanged.

The number of Vitalité health-care workers off the job because of COVID has dropped nearly 55 per cent to 15 in the past month, data released Tuesday shows.
The number of Vitalité health-care workers off the job because of COVID has dropped nearly 55 per cent to 15 in the past month, data released Tuesday shows. (CBC)
Vitalité's COVID outbreaks page hasn't been updated since March 21. At that time, there was one outbreak on Unit 200 at the Veterans' Health Centre in the Moncton region.
A month ago, three hospitals each had one unit with an outbreak.
Horizon Health Network has not yet updated its COVID dashboard.
Yommie
SpeedLimited
- Oct 2, 2013
- 64,204
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #498
Flu continues to grip Ottawa as COVID, RSV levels settle
Flu wastewater readings, hospitalization remain very high
Andrew Foote · CBC News · Posted: Mar 28, 2024 10:34 AM EDT | Last Updated: 1 hour ago
Pedestrians walk along Wellington Street in Ottawa on April 16, 2022, during the sixth wave of the COVID-19 pandemic. (Trevor Pritchard/CBC)
Social Sharing
- X
- Ottawa's COVID-19 and RSV numbers are low to moderate.
- Some flu trends are still seen as very high.
- Three more COVID deaths have been reported.
The latest
The weekly respiratory update from Ottawa Public Health (OPH) is a familiar one.COVID-19 and RSV are seen as low or moderate. Flu wastewater readings and hospitalizations, though dropping, remain very high as this flu season stretches into spring.
Health officials recommend people cover coughs, wear masks, keep hands clean, stay home when sick and keep up with COVID and flu vaccines to help protect themselves and vulnerable people.
OPH says the city's health-care institutions remain at high risk from respiratory illnesses, as they've been since the end of August. This will be the case until respiratory trends are low again.
COVID-19 in Ottawa
Ottawa's coronavirus wastewater average is low and stable.
Researchers have measured and shared the amount of novel coronavirus in Ottawa's wastewater since June 2020. This is the data for the last year. (613covid.ca)
The weekly average test positivity rate in the city is 10 per cent, ticking back up into moderate territory. There are again 14 new COVID-related hospitalizations in the city and the active COVID outbreak count remains at six.
There has been one more COVID death reported in the capital. OPH's next COVID vaccination update is expected in early April.
Across the region
In western Quebec, 18 hospital patients have tested positive for COVID and the region is reporting one more death.The Kingston area health unit is again out of high-risk respiratory territory.
The Eastern Ontario Health Unit (EOHU) still rates its overall respiratory risk as moderate and stable.
Renfrew County's COVID trends are stable, with one more death.
Leeds, Grenville and Lanark (LGL) data goes up to March 17, when its trends were stable or dropping. Hastings Prince Edward (HPE) Public Health hadn't filed its weekly COVID update by publishing time.
Yommie
SpeedLimited
- Oct 2, 2013
- 64,204
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #499
Do you need a spring COVID-19 vaccine? Research backs extra round for high-risk groups
Recent studies suggest staying up-to-date on COVID shots helps protect high-risk groups from severe illness

Lauren Pelley · CBC News · Posted: Mar 28, 2024 4:00 AM EDT | Last Updated: 8 hours ago

Workers prepare doses at a COVID-19 vaccination clinic in Vancouver. New guidelines suggest certain high-risk groups could benefit from having another dose of COVID-19 vaccines this spring. (Ben Nelms/CBC)
Social Sharing
- X
comments
New guidelines suggest certain high-risk groups could benefit from having another dose of a COVID-19 vaccine this spring — and more frequent shots in general — while the broader population could be entering once-a-year territory, much like an annual flu shot.
Medical experts told CBC News that falling behind on the latest shots can come with health risks, particularly for individuals who are older or immunocompromised.
"Even when the risk of infection starts to increase, the vaccines still do a really good job at decreasing risk of severe disease," said McMaster University researcher and immunologist Matthew Miller.
Who needs another COVID shot?
Back in January, Canada's national vaccine advisory body set the stage for another round of spring vaccinations. In a statement, the National Advisory Committee on Immunization (NACI) stated that starting in spring 2024, individuals at an increased risk of severe COVID may get an extra dose of the latest XBB.1.5-based vaccines, which better protect against circulating virus variants.
Quebec has been offering a new vaccine adapted to the new variants since October. (Kristopher Radder/The Associated Press)
That means:
- Adults aged 65 and up.
- Adult residents of long-term care homes and other congregate living settings for seniors.
- Anyone six months of age or older who is moderately to severely immunocompromised.
"Vaccinated people can also pass antibodies to their baby through the placenta and through breastmilk," that guidance states.
What do the provinces now recommend?
Multiple provinces have started rolling out their own regional guidance based on those early recommendations — with a focus on allowing similar high-risk groups to get another round of vaccinations.B.C. is set to announce guidance on spring COVID vaccines in early April, officials told CBC News, and those recommendations are expected to align with NACI's guidance.
In Manitoba, high-risk individuals are already eligible for another dose, provided it's been at least three months since their latest COVID vaccine.
- Older P.E.I. residents, others at risk, urged to get spring COVID vaccine booster
- High-risk groups can now book spring COVID-19 vaccination in Nova Scotia
Having a spring dose "is particularly important for individuals at increased risk of severe illness from COVID-19 who did not receive a dose during the Fall 2023 program," the guidance notes.
And in Nova Scotia, the spring campaign will run from March 25 to May 31, also allowing high-risk individuals to get another dose.
Specific eligibility criteria vary slightly from province-to-province, so Canadians should check with their primary care provider, pharmacist or local public health team for exact guidelines in each area.
WATCH: Age still best determines when to get next COVID vaccine dose, research suggests:

Age still best determines when to get COVID vaccines, new research suggests
17 days ago
Duration1:59
It's been four years since COVID-19 was declared a pandemic, and new research suggests your age may determine how often you should get a booster shot.
Why do the guidelines focus so much on age?
The rationale behind the latest spring guidelines, Miller said, is that someone's age remains one of the greatest risk factors associated with severe COVID outcomes, including hospitalization, intensive care admission and death."So that risk starts to shoot up at about 50, but really takes off in individuals over the age of 75," he noted.
Canadian data suggests the overwhelming majority of COVID deaths have been among older adults, with nearly 60 per cent of deaths among those aged 80 or older, and roughly 20 per cent among those aged 70 to 79.
People with compromised immune systems or serious medical conditions are also more vulnerable, Miller added.

Someone's age remains one of the greatest risk factors associated with severe COVID outcomes, including hospitalization, intensive care admission and death, according to researchers. (Evan Mitsui/CBC)
Will people always need regular COVID shots?
While the general population may not require shots as frequently as higher-risk groups, Miller said it's unlikely there will be recommendations any time soon to have a COVID shot less than once a year, given ongoing uncertainty about COVID's trajectory."Going forward, I suspect for pragmatic reasons, [COVID vaccinations] will dovetail with seasonal flu vaccine campaigns, just because it makes the implementation much more straightforward," Miller said.
- Just 15% of Canadians got updated COVID vaccines this fall, new figures show
- Spring COVID-19 vaccines available April 2 in N.B. for those at high-risk
In the meantime, the guidance around COVID shots remains simple at its core: Whenever you're eligible to get another dose — whether that's once or twice a year — you might as well do it.
What does research say?
One analysis, published in early March in the medical journal Lancet Infectious Diseases, studied more than 27,000 U.S. patients who tested positive for SARS-CoV-2, the virus behind COVID, between September and December 2023.The team found individuals who had an updated vaccine reduced their risk of severe illness by close to a third — and the difference was more noticeable in older and immunocompromised individuals.
Another American research team from Stanford University recently shared the results from a modelling simulation looking at the ideal frequency for COVID vaccines.
- Elderly Canadians remain at higher risk of serious COVID from first infections, study suggests
- Spring vaccine dose suggested to protect seniors in Canada from severe COVID
For younger, healthier populations, however, the benefit of regular shots against severe illness was more modest.
The outcome wasn't a surprise to Stanford researcher Dr. Nathan Lo, an infectious diseases specialist, since old age has consistently been a risk factor for severe COVID.
"It's almost the same pattern that's been present the entire pandemic," he said. "And I think that's quite striking."
More frequent vaccination won't prevent all serious infections, he added, or perhaps even a majority of those infections, which highlights the need for ongoing mitigation efforts.
Yommie
SpeedLimited
- Oct 2, 2013
- 64,204
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #500

WHO launches CoViNet: a global network for coronaviruses
WHO has launched a new network for coronaviruses, CoViNet, to facilitate and coordinate global expertise and capacities for early and accurate detection, monitoring and assessment of SARS-CoV-2, MERS-CoV and novel coronaviruses of public health importance.
WHO launches CoViNet: a global network for coronaviruses
27 March 2024News release
Geneva
Reading time: 1 min (308 words)
WHO has launched a new network for coronaviruses, CoViNet, to facilitate and coordinate global expertise and capacities for early and accurate detection, monitoring and assessment of SARS-CoV-2, MERS-CoV and novel coronaviruses of public health importance.
CoViNet expands on the WHO COVID-19 reference laboratory network established during the early days of the pandemic. Initially, the lab network was focused on SARS-CoV-2, the virus that causes COVID-19, but will now address a broader range of coronaviruses, including MERS-CoV and potential new coronaviruses. CoViNet is a network of global laboratories with expertise in human, animal and environmental coronavirus surveillance.
The network currently includes 36 laboratories from 21 countries in all 6 WHO regions.
Representatives of the laboratories met in Geneva on 26 – 27 March to finalize an action plan for 2024-2025 so that WHO Member States are better equipped for early detection, risk assessment, and response to coronavirus-related health challenges.
The CoViNet meeting brings together global experts in human, animal, and environmental health, embracing a comprehensive One Health approach to monitor and assess coronavirus evolution and spread. The collaboration underscores the importance of enhanced surveillance, laboratory capacity, sequencing, and data integration to inform WHO policies and support decision-making.
“Coronaviruses have time and again demonstrated their epidemic and pandemic risk. We thank our partners from around the world who are working to better understand high threat coronaviruses like SARS, MERS and COVID-19 and to detect novel coronaviruses,” said Dr Maria Van Kerkhove, acting Director of WHO’s Department of Epidemic and Pandemic Preparedness and Prevention. “This new global network for coronaviruses will ensure timely detection, monitoring and assessment of coronaviruses of public health importance.”
Data generated through CoViNet's efforts will guide the work of WHO's Technical Advisory Groups on Viral Evolution (TAG-VE) and Vaccine Composition (TAG-CO-VAC) and others, ensuring global health policies and tools are based on the latest scientific information.
Yommie
SpeedLimited
- Oct 2, 2013
- 64,204
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #501
Want to avoid winter's unwanted house guests? Here's when to get your vaccinations
As the weather starts to cool, now is the time to start preparing for some very unwanted house guests. Here's the latest information about changes to vaccine guidelines, and new immunisations.
 www.abc.net.au
www.abc.net.au
Flu, RSV and COVID cases are set to rise soon, so when should you get vaccinated?
ABC Health & Wellbeing/
By health reporter Paige Cockburn
Posted Tue 26 Mar 2024 at 2:30pmTuesday 26 Mar 2024 at 2:30pm, updated 12h ago12 hours ago
Experts say the best time to get the flu shot is fast approaching.(Getty Images:: Justin Paget)
abc.net.au/news/protecting-yourself-against-flu-rsv-and-covid/103588894
Copy linkLink copied
Share article
Cooler weather is on our doorstep and it's bringing some very unwanted house guests — their names are COVID, influenza and RSV.
Some experts are predicting a particularly bad flu season and there's concern vaccine uptake will remain low and, in turn, hospitalisations will increase.
There's also talk of the dreaded "flu-rona".
Past experience shows RSV infections will ramp up soon too, usually around April. Some vaccine guidelines have also recently changed.
Let's unpack the latest advice.
Influenza
The 2023 flu season was particularly long, but the 2024 season could be even worse, says Michael Clements, vice president and rural chair of the Royal Australian College of GPs."We've been isolated in the past [during the pandemic] so there isn't a lot of herd immunity.
"International travel is full steam ahead and we typically import our influenza from the northern hemisphere."
However, he says a higher rate of infections can also reflect the fact people can now buy at-home testing kits and find out if they have influenza or RSV.
"So in the past we may never have even known they had influenza."
Children aged between six months to five years old are at high risk of developing severe influenza symptoms.(Getty Images: MoMo Productions)
Christopher Blyth, a paediatric infectious diseases professor with the University of Western Australia, says every influenza season is different so it's hard to make many predictions.
"But what I will say is a significant number of children will be hospitalised with influenza this year, like every year."
Last year, children between the ages of five and nine had the highest influenza notification rates, and the number of deaths in children under 16 was higher than in many pre-COVID pandemic years.
"The bulk of children hospitalised are in good health, they just aren't vaccinated," says Professor Blyth, who's the director of the Wesfarmers Centre of Vaccines and Infectious Diseases at the Telethon Kids Institute.
According to the latest government data, influenza cases are higher than expected for this time of year (around 1.7 times greater than the same time last year).
Your immunisation guide:
Annual influenza vaccination is recommended for everyone over six months of age.
The following groups can receive their vaccine for free under the National Immunisation Program (NIP):
- children aged between six months and five years
- those over 65
- Aboriginal and Torres Strait Islander people
- anyone pregnant
- those with medical conditions that increase their risk of severe influenza
Dr Clements says pharmacies are starting to see vaccines trickle in, but the government stock is not due until around early April.
"I know some people are really keen but we actually want to tell them it's OK to wait, as it takes a month or so to get peak effect from the vaccine and it does taper off at between four to six months."
Professor Blyth says getting a vaccine in April will mean you're protected when infections start ramping up in May and still be covered for the peak, which is typically in August.
A flu vaccine is needed every year as influenza virus strains mutate.(ABC News: Herlyn Kaur)
Vaccination coverage last year was low, with around 32 per cent of the population vaccinated.
Dr Clements says it's "heartbreaking" to see people suffer from something preventable and he particularly wants to see more pregnant women and young children vaccinated this year.
He says the higher the vaccine uptake, the lower the peak of infections. This will make the entire community safer, including those who aren't vaccinated.
"Because there's always people who can't get the vaccine or have it but it doesn't work."
The vaccine's effectiveness rate is between 40 to 60 per cent.
RSV
Respiratory syncytial virus (RSV) infections are common and can be very disruptive."Most parents can give a really good history of being awake at night worried about the wet cough their child has," Dr Clements says.
"For the elderly, it's often RSV that triggers the pneumonia that kills them."
Chronic cough should be investigated, say doctors
A cough is necessary to keep the airways clear and to remove foreign particles such as dust. But respiratory experts say coughs that linger need to be investigated.Read more
The virus can infect the lungs and breathing passages and is the leading cause of hospitalisations in infants nationwide.
RSV is so common partly because individuals lose their immunity to it relatively quickly. Reinfection can occur just two months after the last infection.
"In the next couple of weeks to months we will have plenty of RSV. It's one of the major causes of bed block in paediatric hospitals," Professor Blyth says.
RSV normally surges around April to July in the southern states, while case numbers in the tropics can be more consistent throughout the year.
Your immunisation guide:
For years, Australians have suffered through RSV without the option of immunisation.
But this autumn, for the first time, that's no longer the case for some people.
The Therapeutic Goods Administration (TGA) last year approved a drug called Nirsevimab, which is a long-acting antibody that's been shown to reduce infections by about 75 per cent for up to five months.
While Nirsevimab is not currently part of the National Immunisation Program (NIP), some states have free immunisation programs for infants and children.
Earlier this month, the Western Australian government announced it will provide free access to Nirsevimab from April for all babies under eight months (or up to 19 months for those at increased risk of severe RSV).
This week, the Queensland and New South Wales governments followed suit and announced their own free RSV immunisation programs.
In Queensland, newborn infants, Aboriginal and Torres Strait Islander infants less than eight months of age and certain infants with complex medical conditions are eligible.
In New South Wales, premature babies born after October 31, 2023, all Aboriginal and Torres Strait Islander babies born after October 31, 2023 and certain vulnerable infants are covered.
WATCH
Duration: 6 minutes 48 seconds6m
Calls for national rollout of free vaccination against RSV.
In a separate development, Australians over the age of 60 may have access to a free RSV vaccine in the future.
The TGA recently approved AREXVY which is a protein-based vaccine for the prevention of lower respiratory tract disease caused by RSV.
It is currently only available on private prescription (which means the consumer pays the full cost) as it's not funded through the NIP.
However the manufacturer of AREXVY has applied for the vaccine to be made available for free through the NIP, and Dr Clements believes this could happen next year.
COVID-19
COVID-19 transmission is low at the moment, Professor Blyth says, but cases are expected to rise around the same time as the influenza and RSV peaks."We're concerned COVID will just piggyback onto another cough or cold so if someone has RSV they might then happen to get COVID and have dual infections and be even sicker," Dr Clements says.
"It's known as flu-rona".
Professor Blyth says those who will be most at risk will be older Australians and those who are immunocompromised.
ABC Health in your Instagram feed
Follow @abchealth on Instagram, where we're busting myths and sharing practical, smart health advice.Read more
Your immunisation guide:
Last month the government updated its COVID-19 vaccination guidelines.
Six-monthly boosters are now only recommended for those over the age of 75.
Anyone over 18 can have an annual booster.
But if you're 65 to 74 or severely immunocompromised you can have a six-monthly booster. Talk to your doctor about the risks and benefits.
A booster is not currently recommended for those between the ages of five and 17 who are not immunocompromised.
Individuals in this age group who are severely immunocompromised can get a booster every 12 months.
Children under five are not currently recommended to have a booster.
Anything else?
Both Dr Clements and Professor Blyth urge all Australians to check with their GP about whether they're up to date with routine vaccinations.This includes the shingles vaccination, which is free under the National Immunisation Program (NIP) for those most at risk, including anyone over the age of 65 or under 18 who is immunocompromised.
New shingles jab free for older Australians
The risk of developing shingles increases with age. But a new vaccine, tipped to be 90 per cent effective, is now available through the National Immunisation Program for older and immunocompromised Australians.Read more
The pneumococcal vaccine is another important one.
Pneumococcal disease can cause a variety of diseases, like pneumonia and meningitis, and young children and the elderly are most at risk.
It is free under the NIP for certain groups including children, adults aged 70 and over and Aboriginal and Torres Strait Islanders aged 50 and over.
"It's not just about protecting yourself against the seasonal viruses but it's about keeping up to date with the routine stuff too," Professor Blyth says.
Editor's note: An earlier version of this story said anyone over the age of 18 was advised to have an annual COVID-19 vaccine booster. This has been amended to better reflect the health advice which says those over 18 (as well as severely immunocompromised individuals aged between 5 –17 years) can receive an annual booster.
Yommie
SpeedLimited
- Oct 2, 2013
- 64,204
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #502

Why, as a doctor, I'd fork out £99 for a private Covid jab
I've had the jab for free as a frontline NHS worker, but otherwise I'd be logging on to the Boots website and booking the vaccine as soon as possible, writes Professor Rob Galloway.
I'm a doctor who knows Covid is usually little worse than a cold - but I'd still fork out £99 for the new private jab. And my reasons will convince you too...
By PROFESSOR ROB GALLOWAYPUBLISHED: 13:17 EDT, 26 March 2024 | UPDATED: 13:55 EDT, 26 March 2024
587
View comments
+99
Home
587
View comments
Have you heard the good news about Covid jabs? It's been reported that from April 1 anyone over the age of 12 will be able to pay to have one at Boots.
At £98.95, they're not cheap, but finally people in this country will be able to get the booster privately, as they can already in the US.
Actually, I don't think in principle any of us should have to pay for jabs against widespread disease such as Covid.
But for its own reasons, the Government has decided to limit who the jab is offered to - and if you're one of the millions of people left out of the current Covid vaccination programme, then £100, in my view, is an investment that you should make if you can afford to.
I've had the jab for free as a frontline NHS worker, but otherwise I'd be logging on to the Boots website and booking the vaccine as soon as possible.
Over the top? You might think so, given that Covid is becoming less virulent, and the initial reasons for getting the vaccine were to stop acute illness.

+1
View gallery
TRENDING

Experts' incredible top tips for warding off dementia
1.8k viewing now

Revealed: The meal deals with the MOST calories
276 viewing now
How a break up can drive you to point of insanity
1.2k viewing now
And the fact is, for healthy people a Covid infection isn't going to be much worse than a cold. So that's a lot of money to spend to stop 'just a cold'.
But I don't think getting the vaccine is about the actual illness and symptoms - it's the single dose Pfizer jab that's on offer, and the evidence shows that this is the most effective vaccine in protecting you against what really worries me as a doctor: long Covid.
That's why I think anyone who hasn't had the Covid booster this year should consider paying for it. And, just to be clear, I do not own shares nor work for Pfizer (or Boots); my only vested interest is in seeing fewer patients come to my A&E department with symptoms.
Like any vaccine, the Covid jab does have potential side effects. And it's clearly not guaranteed to stop infection entirely – no vaccine can.
If the pandemic hadn't happened, of course I wouldn't want the vaccine, especially one developed so quickly and without the reassurance of the long-term safety data that there is for other more established vaccines.
But the fact is that, post-pandemic, Covid will continue to circulate in the community and continue to infect us all at regular intervals for many years to come.
And looking at the data from independent studies, this has shown that the benefits massively outweigh the potential harms, not just in reducing your chances of getting Covid, and the severity of the infection, but crucially, in reducing your chances of developing long Covid.
There is no doubt that long Covid is a genuine health problem, and I've seen too many previously healthy people floored by it to risk getting it myself. Its list of awful symptoms range from brain fog to heart problems, to fatigue and repeated infections. It's very much not 'all in the mind' as some suggest – people with long Covid can experience a reduction in brain volume (as seen in MRI scans) and impaired immune response to infections (as shown on blood tests).
On a recent shift, I saw a previously well woman in her 20s come into A&E after she'd suddenly collapsed – six months previously she'd caught Covid, and she'd never recovered. She'd had to stop working because of fatigue and her weekly 5km park runs were a thing of the past.
READ MORE: How more vitamin C could transform your mood and slow cognitive decline - and here are the best foods to load up on it
She'd also developed POTS (Postural orthostatic tachycardia syndrome) and frequently collapsed because her heart rate becomes dangerously high when she stands up. This time she'd cut her head when she fell – I was able to sort that out quickly with stitches, but there are no quick fixes for her long Covid.
So the question is, can the vaccines prevent Covid and long Covid? The answer is 'yes' and 'yes', as shown in a number of studies and confirmed in a robust and major new piece of research, published in the journal Lancet Respiratory Medicine in January this year.
The researchers looked at GP databases involving more than 20million patients from various countries around Europe and the UK. They found that if you had a Covid vaccine, it reduced your chances of getting long Covid by 46 per cent. In addition, the study showed that the Pfizer vaccine was more effective than the Oxford/AstraZeneca vaccine in preventing long Covid.
Although it's not the 'perfect' study (which would involve giving participants either a vaccine or a placebo and comparing long Covid rates), it's the best possible and most ethically feasible study you could conduct in the real world.
The results not only showed a massive benefit of the vaccine for preventing long Covid, but the results were proven beyond statistical doubt.
But maybe you think long Covid isn't that much of a worry and only a few people get it... Well, let me remind you that the evidence shows even mild Covid can lead to long Covid.
And when it comes to the numbers, about 2 per cent of the population who haven't had the vaccine get long Covid. But by having a vaccine, we can reduce that risk of long Covid by half to 1 per cent.
In my view, that cut makes a £100 vaccine a good investment. After all, I have taken out house insurance though the chances of my house burning down are much lower than 1 per cent. Similarly, I have insurance for my car and, contrary to my wife's opinion of my driving, my chances of a car accident are less than 1 per cent.
So why not pay £100 for long Covid insurance?
But for me, the key question is why is the jab so expensive privately - and shouldn't the NHS be paying for everyone anyway?
I hope the take-up for the private jab will be high, but that will create a two-tier level of health, with those who can afford the vaccine having much lower levels of long Covid than those who can't afford it. This is unfair and unjust.
The sad truth is that we live in an unfair and unjust world. And when it comes to our health and the health of our loved ones, my moral conviction that such jabs should be free for all would be trumped by my desire to reduce the chance of ill-health among my family and friends.
Finally, if you are considering getting the vaccine to reduce your risks of long Covid, also consider what else you can do to prevent it or minimise the severity: Covid rates are so much lower in non-smokers, moderate drinkers, those who have a balanced diet, who regularly exercise and are a healthy weight.
Either way, yone thing is for certain: you really don't want to get long Covid.
Professor Rob Galloway is an A&E consultant
Yommie
SpeedLimited
- Oct 2, 2013
- 64,204
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #503

Major change to Covid testing will kick in next week
It means the new system in England, enforced from April 1, will only see free tests provided to at-risk staff and residents with symptoms.
Now it's REALLY the end of the Covid era! Routine lateral flows for patients being discharged from hospitals into care homes will be axed next week
- Testing for asymptomatic patients moving into care settings will end from April 1
- READ MORE: Why going into hospital can be VERY bad for your health
PUBLISHED: 13:32 EDT, 25 March 2024 | UPDATED: 14:08 EDT, 25 March 2024
206
View comments
+99
Home
206
View comments
Routine lateral flow testing for Brits discharged from hospitals into care homes will be axed from next week.
Under the Government's 'living with Covid' blueprint, the shift is designed to bring guidance in line with other respiratory illnesses like flu.
Ministers today argued the threat of the virus has been drastically reduced by the wall of immunity built up by vaccines and infections.
It means the new system in England, enforced from April 1, will only see free tests provided to some groups, including staff on inpatient wards treating immunocompromised individuals.
Experts, however, warned that axing the policy could have 'serious consequences'.

+4
View gallery
TRENDING
Experts' incredible top tips for warding off dementia
1.7k viewing now

Will conjoined twin Abbey Hensel now realize dream of being a mother?
21.6k viewing now

Stephen Bear ordered to pay £27,500 over Georgia Harrison sex tape
10.1k viewing now
Health minister Maria Caulfield said: 'Given the high levels of vaccination among groups at higher risk, wider access to treatments and reduced impact of outbreaks, the Government is now able to remove some of the highly targeted testing which remains in place from the height of the pandemic.
'Due to a combination of immunity acquired from natural infection or vaccination, Covid is now a relatively mild disease for the vast majority of people.'
NHS trusts will have 'local discretion' to reintroduce Covid testing 'as clinically appropriate following risk assessment', she added.
Care providers and hospices 'will also continue to have the ability to discuss and raise any concerns about discharge arrangements through existing local mechanisms', she said.
Seven in 10 people aged over 65 living in England and eight in 10 care home residents had a Covid booster last autumn, figures suggest.

+4
View gallery

+4
View gallery
Care England, a representative organisation for small, medium and large providers across the country, urged the Government to continue testing.
Professor Martin Green, its chief executive, said: 'People who live in care homes are often living with many health conditions and are susceptible to infectious diseases.
'It is for this reason that we would like to see testing continue when patients are being discharged from hospital.
'If we see an end to such testing, the risk of people coming from hospital with asymptomatic Covid and transmitting it to other residents could have serious consequences.'
Failures to test patients who were discharged into care homes at the start of the pandemic remains one of Government's most controversial Covid measures.
During the earliest days of the pandemic, homes in England were made to accept patients who hadn't been swabbed for the virus in a desperate attempt to free up NHS beds.
Thousands of care home residents are feared to have died as a direct result of the disastrous policy.
This is despite claims from disgraced ex-Health Secretary Matt Hancock, who resigned after being caught kissing an aide in breach of Covid guidelines, that ministers had thrown a 'protective ring' around care homes.
Last year, Dame Jenny Harries — now head of the UK Health Security Agency — also told the Covid inquiry that discharging Covid-infected NHS patients into care homes was 'entirely clinically appropriate'.
Yommie
SpeedLimited
- Oct 2, 2013
- 64,204
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #504

One state set to scrap Covid vaccine mandates
Vaccine mandates for NSW health workers could soon be dropped as the state government weighs up lifting the Covid pandemic-era requirements.
Mandatory Covid vaccines set for the axe in New South Wales after health chief Dr Kerry Chant softens on ban
- NSW could drop the Covid vaccine mandate for health workers
- Health Minister Ryan Park confirmed the change is being considered
- READ MORE: Australians struck down with Covid warned to 'stay at home'
PUBLISHED: 17:28 EDT, 24 March 2024 | UPDATED: 21:57 EDT, 24 March 2024
View comments
+99
Home
Vaccine mandates for NSW health workers could soon be dropped as the state government weighs up lifting the Covid-19 pandemic-era requirements.
Health Minister Ryan Park confirmed the change would be considered after consulting with the state's health workforce.
'We know that Covid is still around but we've got to get back on with life,' he told Sydney radio 2GB on Monday.
'That means having a look at the measures we put in place during this period and seeing whether they still apply.
'We think this is one that we can engage with the workforce on and have a look to see if it's still applicable now.'

+3
View gallery
TRENDING

Urgent search for girl who vanished from daycare in Sydney yesterday
35.4k viewing now

Woman launches rant at family during river boat trip... then capsizes
68.2k viewing now
Three-time gangster WAG ties the knot with Alameddine associate
1.4k viewing now
NSW chief health officer Kerry Chant said if consultation led to mandate changes, workers would continue to be strongly recommended to stay up to date with their vaccinations.
'Covid-19 vaccination continues to provide strong protection against severe illness, particularly for people at higher risk of serious illness and death from Covid-19, including older adults and those with underlying health conditions,' she said.
'While the latest evidence shows most people have now developed protection from serious disease due to vaccination and/or previous infection, Covid-19 remains a serious public health issue.'
Orders mandating vaccines for all health-care workers were introduced in August 2021 and staff who refused to comply either quit or were sacked.
Mr Park said if a decision was made to drop the mandates, workers who lost their jobs would be able to reapply to available positions through the usual recruitment processes.
He said Covid-19 was still a public health threat and encouraged people to keep up with their vaccinations.

+3
View gallery
'But we've also got to make sure that we get on with running a health system after Covid and we can't continue in the same way that we did in the middle of the pandemic,' he said.
Current advice from the Australian Technical Advisory Group on Immunisation is a vaccine dose every six months for people aged 75 years and over and every 12 months for people aged 65 to 74 years.
Immunocompromised people can consider having a vaccine every six months, while all other adults between the ages of 18 to 64 should consider a vaccine dose every 12 months.
Yommie
SpeedLimited
- Oct 2, 2013
- 64,204
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #505
Australia: Queensland’s chief health officer calls for the scrapping of the term “Long COVID”
Gerrard’s assertion is part of the campaign by the political establishment in Australia to normalise COVID-19 with the claim that Long COVID is no different to the long-term symptoms of seasonal influenza.
www.wsws.org
Australia: Queensland’s chief health officer calls for the scrapping of the term “Long COVID”
Frank Gaglioti
43 minutes ago
In a press conference on March 15, Queensland’s Chief Health Officer Dr John Gerrard used a study that will be presented at the European Congress of Clinical Microbiology and Infectious Diseases in Barcelona in April to cast doubt on the term Long COVID as a distinct condition.Queensland Chief Health Officer Dr John Gerard [Photo: ABC-TV screenshot]
“What we are saying is that the incidence of these symptoms is no greater in COVID-19 than it is with other respiratory viruses, and that to use this term ‘long COVID’ is misleading and I believe harmful,” Gerrard said.
Gerrard’s assertion is part of the campaign by the political establishment in Australia to normalise COVID-19 with the claim that Long COVID is no different to the long-term symptoms of seasonal influenza.
The World Socialist Web Site correctly called the pandemic a mass disabling event. In what is a vast undercount, according to the worldmeter website 704 million people have been infected and seven million have died. However, measures of excess deaths put the toll at 28 million. In Queensland there have been 1.8 million people infected with 3,375 dying. The most conservative estimate is that 10 percent of the infected cohort will develop Long COVID.
Gerrard and his group’s study surveyed 5,112 adults who had respiratory infections in May and June 2022, at the height of the Omicron surge. Polymerase chain reaction tests (PCR) were used to identify that there were 2399 who had COVID-19, 995 had influenza and 1,718 were negative for both. In the infected cohort, 16 percent had symptoms a year later, while 3.6 percent reported moderate to severe symptoms.
Their study found that 3 percent of the COVID-19 patients had ongoing impairment while 3.4 percent of influenza patients had ongoing issues.
Gerrard concluded that “We believe it is time to stop using terms like ‘long COVID.’ They wrongly imply there is something unique and exceptional about longer-term symptoms associated with this virus. This terminology can cause unnecessary fear, and in some cases, hypervigilance to longer symptoms that can impede recovery.”
While the study has not yet been published or peer reviewed, an outline of his findings has been published in the mainstream media. The story was embargoed until March 15, dubbed #LongCovidAwarenessDay, representing a slap in the face for the millions of sufferers internationally.
Gerrard’s study, funded by Queensland Health that he heads, is very limited in its scope and his findings have no veracity.
The methodology is highly suspect. It only used a very small sample size of 2,713 people and relied on the participants’ subjective assessment of their condition. He eliminated a number of people on unclear grounds. The study was conducted via SMS and the subjects were not examined or interviewed. The subjects were simply asked questions via text message.
Director of the Australian National Phenome Centre at Murdoch University Professor Jeremy Nicholson told the Guardian the question of whether long COVID is unique “cannot be simply answered in this work. The study is observational, based on reported symptoms with no physiological or detailed functional follow-up data. Without laboratory pathophysiological assessment of individual patients, it is impossible to say that this is indistinguishable from flu-related or any other post-viral syndrome.”
Moreover, according to reports of the study, the symptoms examined by text were also limited and included fatigue, post exertional symptom exacerbation, brain fog and changes to taste and smell. This is insufficient in drawing out the differences between Long COVID, which can affect every organ of the body, and Long influenza. Both conditions are caused by viral infections, but they impact on the body in quite different ways.
Some of the most prevalent symptoms of Long COVID
The study and Gerrard’s conclusions are politically motivated and aimed at sidelining Long COVID as a distinct condition under conditions where governments, state and federal, have ended virtually all much-needed COVID restrictions.
Nephrologist at Campbelltown Hospital Dr Satoshi Akima posted on X/Twitter: “Even if the incidence of post-viral syndromes is the same after all viral infections, this is not grounds to gaslight, but to take all post-viral syndromes infinitely more seriously.”
Despite the media downplaying the coverage of COVID generally, this study has been widely reported internationally and may form the basis for justifying the dismantling of the very limited Long COVID measures in place.
An earlier version of Gerrard’s study published in the BMJ (British Medical Journal) in August 2023 “Ongoing symptoms and functional impairment 12 weeks after testing positive for SARS-CoV-2 or influenza in Australia: an observational cohort study.”
It was essentially the same study, using the same people as subjects but following them up after only 12 weeks, a very short time for the full extent of the conditions to emerge. The participants responded to three questions on the impact of their condition, making any serious assessment their infection impossible.
Yet Gerrard draws almost identical conclusions in both versions. “In a highly vaccinated population exposed to the SARS-CoV-2 Omicron variant, long COVID may manifest as a postviral syndrome of no greater severity than seasonal influenza but differing in terms of the volume of people affected and the potential impact on health systems,” the 2023 study stated.
Gerrard is a crass proponent of herd immunity. In December 2021, at the start of the Omicron surge, government authorities in Australia and internationally used the new variant’s emergence to eliminate the limited mitigation programs in place. Without a shred of evidence, they pronounced Omicron less virulent.
In December 2021, Gerrard told the Australian Broadcasting Corporation (ABC): “In order for us to go from the pandemic phase to an endemic phase, the virus has to be widespread. We all have to have immunity [and] there’s two ways you can do that—by being vaccinated or getting infected. Once we’ve done that, once the virus is spreading, once we all have some degree of immunity, the virus becomes endemic and that is what is going to happen.”
This was a cruel hoax and was used as the pseudo-scientific argument to ignore the virus’s existence as it continued to proliferate, mutating into variants able to evade human immunity more effectively.
Gerrard’s work is in line with the far-right’s campaign to liken COVID-19 to the seasonal flu. Figures such as the former Brazilian President Jair Bolsonaro called COVID-19 a “little flu.”
MEHRING BOOKS
COVID, Capitalism, and Class War: A Social and Political Chronology of the Pandemic
A compilation of the World Socialist Web Site's coverage of this global crisis, available in epub and print formats.
BUY YOUR COPY TODAY
This claim was definitively disproved in a landmark study led by Dr. Ziyad Al-Aly, the director of the Clinical Epidemiology Center, chief of research and development service at the Veterans Affairs (VA) Saint Louis Health Care System. The research was published in the Lancet on 14 December 2023, “Long-term outcomes following hospital admissions from COVID-19 versus seasonal influenza: a cohort study.”
While Al-Aly did not intend it as such, his group’s paper represents a devastating rebuttal of Gerrard’s comments and his study. It involved a far greater number of patients than Gerrard did, and was conducted in a far more systematic manner.
Dr. Al-Aly and his group used the data from the Veterans Affairs (VA) Saint Louis Health Care System to compare 82,000 patients who had been admitted for COVID-19 between March 1, 2020, and June 30, 2022 to an historical group of influenza sufferers between October 1, 2015, and February 28, 2019 of nearly 11,000 influenza patients who had been hospitalised, for a comparison group. An historical group was used for influenza as the virus had been almost eliminated due to COVID mitigation measures.
Dr. Al-Aly at his desk [Photo by Dr. Ziyad Al-Aly]
Importantly the group examined 94 health measures encompassing 10 organ systems. It analysed “cardiovascular, coagulation and hematological, fatigue, gastrointestinal, kidney, mental health, metabolic, musculoskeletal, neurological, and pulmonary” symptoms over an extended period of 18 months.
Over the 18-month period, COVID-19 was associated with “significant increased risk” in 64 of the 94 measured health outcomes that encompassed nearly every organ system in the human body. By comparison, seasonal influenza was only associated with increases in six of the 94 health outcomes that included, angina, tachycardia, type 1 diabetes, and three pulmonary outcomes (cough, hypoxia, and shortness of breath).
In a communication with the World Socialist Web Site, Dr Al-Aly concluded: “We observed higher risks of death, healthcare utilization and hits in most organ systems in COVID-19 than the flu… COVID-19 remain a much more serious threat to human health than the flu.”
He added that the study findings underscored that “COVID-19 is really a multisystemic disease and flu is more of a respiratory virus… The burden of health loss from Long-Flu is substantial, but the burden of health loss from Long-COVID-19 is even higher. Yet, both Long-COVID-19 and Long-Flu lead to more health loss than either acute COVID-19 or Flu. Conceptualizing these illnesses as acute events obscures the much larger burden of health loss that occurs in the post-acute phase.” [Emphasis added]
A number of scientists, doctors and long COVID patients have specifically opposed Gerrard’s claims which have also drawn myriad criticisms via social media. His pseudo-scientific claims represent an attack on the millions of sufferers of Long COVID internationally. This condition was brought to the attention of the medical and scientific fraternity by Long COVID sufferers, dubbing themselves “long haulers.”
Leading Long COVID advocate Dr. Elisa Perego, who first coined the hashtag #LongCovid in May 2020 after her experience with prolonged symptoms posted a searing indictment of Gerrard’s work on X: “The very same term #LongCovid is an existential threat for people who told their citizens that getting infected was a way to immunity, that infection with SARS-CoV-2 (the virus that causes COVID-19) was necessary and desirable… They *did* it for real.”
Respiratory physician at Royal North Shore Hospital in Sydney Dr. David Joffe summarised the criticisms posting on X: “I think you would cringe at the methodology and statistical evaluation. It’s unpublished, non-peer reviewed. Based on a text response, and excluded many candidate subjects. Long C-19 Awareness Day—March 15. This is an attempt to trivialise a serious disease.”
The fact that a figure such as Gerrard is selected to oversee the public health of Queensland demonstrates that the political establishment has completely renounced any measures to mitigate the pandemic or treat the millions who suffer from Long COVID. His study was seized upon by the corporate media to further justify the policy that governments everywhere have adopted.
Yommie
SpeedLimited
- Oct 2, 2013
- 64,204
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #506

Number hospitalized with COVID-19 in B.C. hits new low for 2024 in latest update
The number of patients with COVID-19 in B.C. hospitals declined to its lowest level of 2024 in the latest data update from the B.C. Centre for Disease Control.
Number hospitalized with COVID-19 in B.C. hits new low for 2024 in latest update


Ian Holliday
CTVNewsVancouver.ca Journalist
Contact
Published March 28, 2024 7:41 p.m. EDT
Share
- Link
- X
There were 133 test-positive patients in provincial hospitals as of Thursday, according to the BCCDC. The last published update to show a total lower than that was in August of last year, when the BCCDC reported just 76 patients hospitalized.
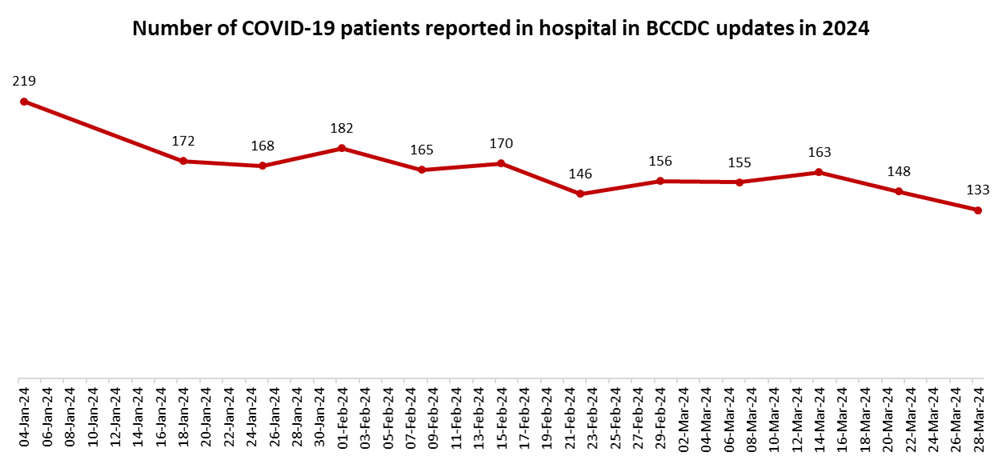
This week's hospitalized population is less than half of what it was around this time last year. The final published update of March 2023 showed 294 patients in B.C. hospitals.
RELATED STORIES
- Anti-vax protester's 'race-based tirade' against security guard wasn't criminal, B.C. judge rules
- COVID-19 hospitalizations drop in weekly BCCDC update
- COVID was a good chance to study what the animals did while humans were locked down
Other data released Thursday by the BCCDC also showed a declining trend. There were 320 new lab-confirmed infections during the most recent "epidemiological week," which spanned March 17 to 23. That's down from 394 during the preceding week.
The percentage of tests coming back positive also declined during the week that ended March 23. Test positivity was 9.7 per cent, down from 10.9 per cent the week before, according to BCCDC data.
These declines in testing-related data are matched by recent declines in concentrations of the SARS-CoV-2 virus at wastewater facilities around the province. Wastewater data can be found on the BCCDC website(opens in a new tab).
Data on other respiratory viruses released Thursday(opens in a new tab) was incomplete. The BCCDC said testing data from both the Fraser and Northern health authorities was "unavailable" for the week of March 17 to 23, but did not explain why.
Yommie
SpeedLimited
- Oct 2, 2013
- 64,204
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #507
Antibody discovery could explain mysteries about COVID-19 and long COVID
UVA Health researchers have discovered a potential explanation for some of the most perplexing mysteries of COVID-19 and long COVID.
 www.news-medical.net
www.news-medical.net
Antibody discovery could explain mysteries about COVID-19 and long COVID


" style="box-sizing: border-box; background-color: transparent; color: rgb(95, 95, 95); text-decoration: none; transition: all 0.15s ease-out 0s; cursor: pointer; border: 0px; overflow-wrap: break-word;">Reviewed
Mar 28 2024University of Virginia Health System
UVA Health researchers have discovered a potential explanation for some of the most perplexing mysteries of COVID-19 and long COVID. The surprising findings could lead to new treatments for the difficult acute effects of COVID-19, long COVID and possibly other viruses.
Researchers led by UVA's Steven L. Zeichner, MD, PhD, found that COVID-19 may prompt some people's bodies to make antibodies that act like enzymes that the body naturally uses to regulate important functions – blood pressure, for example. Related enzymes also regulate other important body functions, such as blood clotting and inflammation.
Doctors may be able to target these "abzymes" to stop their unwanted effects. If abzymes with rogue activities are also responsible for some of the features of long COVID, doctors could target the abzymes to treat the difficult and sometimes mysterious symptoms of COVID-19 and long COVID at the source, instead of merely treating the downstream symptoms.
Some patients with COVID-19 have serious symptoms and we have trouble understanding their cause. We also have a poor understanding of the causes of long COVID. Antibodies that act like enzymes are called 'abzymes.' Abzymes are not exact copies of enzymes and so they work differently, sometimes in ways that the original enzyme does not. If COVID-19 patients are making abzymes, it is possible that these rogue abzymes could harm many different aspects of physiology. If this turns out to be true, then developing treatments to deplete or block the rogue abzymes could be the most effective way to treat the complications of COVID-19."
Steven L. Zeichner, MD, PhD, pediatric infectious disease expert at UVA Children's
Understanding COVID-19 abzymes
SARS-CoV-2, the virus that causes COVID, has protein on its surface called the Spike protein. When the virus begins to infect a cell, the Spike protein binds a protein called Angiotensin Converting Enzyme 2, or ACE2, on the cell's surface. ACE2's normal function in the body is to help regulate blood pressure; it cuts a protein called angiotensin II to make a derivative protein called angiotensin 1-7. Angiotensin II constricts blood vessels, raising blood pressure, while angiotensin 1-7 relaxes blood vessels, lowering blood pressure.Zeichner and his team thought that some patients might make antibodies against the Spike protein that looked enough like ACE2 so that the antibodies also had enzymatic activity like ACE2, and that is exactly what they found.
Recently, other groups have found that some patients with long COVID have problems with their coagulation systems and with another system called "complement." Both the coagulation system and the complement system are controlled by enzymes in the body that cut other proteins to activate them. If patients with long COVID make abzymes that activate proteins that control processes such as coagulation and inflammation, that could explain the source of some of the long COVID symptoms and why long COVID symptoms persist even after the body has cleared the initial infection. It also may explain rare side effects of COVID-19 vaccination.
To determine if antibodies could be having unexpected effects in COVID patients, Zeichner and his collaborators examined plasma samples collected from 67 volunteers with moderate or severe COVID on or around day 7 of their hospitalization. The researchers compared what they found with plasma collected in 2018, prior to the beginning of the pandemic. The results showed that a small subset of the COVID patients had antibodies that acted like enzymes.
 SLAS EU - Highlights from 2022 eBook Compilation of the top interviews, articles, and news in the last year.Download the latest edition
SLAS EU - Highlights from 2022 eBook Compilation of the top interviews, articles, and news in the last year.Download the latest editionWhile our understanding of the potential role of abzymes in COVID-19 is still in its early stages, enzymatic antibodies have already been detected in certain cases of HIV, Zeichner notes. That means there is precedent for a virus to trigger abzyme formation. It also suggests that other viruses may cause similar effects.
Zeichner, who is developing a universal coronavirus vaccine, expects UVA's new findings will renew interest in abzymes in medical research. He also hopes his discovery will lead to better treatments for patients with both acute COVID-19 and long COVID.
"We now need to study pure versions of antibodies with enzymatic activity to see how abzymes may work in more detail, and we need to study patients who have had COVID-19 who did and did not develop long COVID," he said. "There is much more work to do, but I think we have made a good start in developing a new understanding of this challenging disease that has caused so much distress and death around the world. The first step to developing effective new therapies for a disease is developing a good understanding of the disease's underlying causes, and we have taken that first step."
Findings published
The researchers have published their findings in the scientific journal mBio, a publication of the American Society for Microbiology. The research team consisted of Yufeng Song, Regan Myers, Frances Mehl, Lila Murphy, Bailey Brooks, and faculty members from the Department of Medicine, Jeffrey M. Wilson, Alexandra Kadl, Judith Woodfolk."It's great to have such talented and dedicated colleagues here at UVA who are excited about working on new and unconventional research projects," said Zeichner.
Zeichner is the McClemore Birdsong Professor in the University of Virginia School of Medicine's Departments of Pediatrics and Microbiology, Immunology and Cancer Biology; the director of the Pendleton Pediatric Infectious Disease Laboratory; and part of UVA Children's Child Health Research Center.
The abzyme research was supported by UVA, including the Manning Fund for COVID-19 Research at UVA; the Ivy Foundation; the Pendleton Laboratory Fund for Pediatric Infectious Disease Research; a College Council Minerva Research Grant; the Coulter Foundation; and the National Institutes of Health's National Institute of Allergy and Infection Diseases, grant R01 AI176515. Additional support came from the HHV-6 Foundation.
Yommie
SpeedLimited
- Oct 2, 2013
- 64,204
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #508

Long Covid makes exercise a challenge, doctors say
Bay Area doctors say people suffering from Long Covid struggle to stay active, potentially causing further health issues.
Yommie
SpeedLimited
- Oct 2, 2013
- 64,204
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #509

Young people like me are still feeling the effects of Covid – and they’re not all bad | Isabel Brooks
Some fared better than others. But the pandemic left its mark on all of us, whether we realise it or not, says freelance writer Isabel Brooks
 www.theguardian.com
www.theguardian.com
Young people like me are still feeling the effects of Covid – and they’re not all bad
Isabel Brooks
When it comes to studies, work or social abilities, some fared better than others. But the pandemic left its mark on all of us, whether we realise it or not
Fri 29 Mar 2024 08.00 GMT
Share
171
Irecently came across a folder on my laptop labelled “Covid”. Inside I found screenshots I had taken of the government website, showing daily cases, ICU admissions and deaths from Covid-19. These reports were released every weekday during the first lockdown, and each afternoon I would collect them in this folder and study them, trying to understand what was happening in the wider world – before I began a busy evening of Zoom birthday quizzes, Netflix Party and WhatsApp.
I was shocked – both that I had ever been so macabre in the first place, and also that, four years later, I had forgotten doing it. I don’t remember being anxious or depressed during lockdown, but I have 60 image files suggesting otherwise.
In general, studies since 2020 have displayed a widespread decline in young people’s mental health, often linked to the experience of the pandemic. According to the Royal College of Paediatrics and Child Health, 75% of mental health difficulties start before the age of 24; so young people are more vulnerable, as adolescence involves crucial milestones in emotional and social development. Some experts claim that my generation may have to suffer the consequences of social distancing and cessation of work for the rest of our lives, that on top of economic difficulties we also face a unique experience of social disintegration.
And yet, despite what my folder of screenshots may suggest, I don’t feel too badly affected by the pandemic. I was 21 and studying at university when Covid hit, and was able to move home for my final exams. I was lucky to have a quiet room to myself, with no financial concerns or specific health issues. Those a couple of years younger than me – starting their studies, rather than finishing them – fared worse, continuing a larger stretch of their university period under the doomscape of 2020 and 2021.
A friend, who is now 22, thinks her peers rely more on “internet speak”, having been immersed in social media over Covid, and thus developed the lexicon and mannerisms from TikTok et al without intention. They also are “much less inclined to go out and drink” and don’t know how to behave in front of “new people”. She told me that, in comparison, 25-year-olds have “more real-life personalities”, which we forged away from our smartphones, before the pandemic.

‘Some experts claim that my generation may be reaping the consequences of social distancing and cessation of work for the rest of our lives.’ Photograph: Alex Cambero/Getty Images/iStockphoto
My darkest point was when I got Covid, just before Christmas 2020. I spent the next fortnight alone, trying to recover, not once leaving the house, or taking a shower. On Christmas Day, I watched 10 episodes of Bridgerton just so I wouldn’t have to sit for a second with my own thoughts. I was struggling. But after I recovered, I was grateful for tiny things, like getting to walk on the grass and have dinner with my family. For a few days, I felt simply happy.
Everyone’s experience was different. Some had worse experiences with the virus itself. Some contracted long Covid, or lost a loved one to it. But such things aren’t restricted to one age group. And so the generational lens may be a blunt tool by which to make assessments; it could be damning to label a whole cohort as psychologically and economically scarred. It is perhaps another way of underestimating young people. After all, those who were most affected across all generations were those who were already at risk of unemployment, mental health issues and poverty. All the stats say that Gen Z has been wounded by the pandemic, but many of my peers are more resilient than people may think.
It’s true that I was affected in terms of personal life and employment, especially in my struggle to get a job after university. I also blame Covid-19 for the breakdown of a past relationship. My then-boyfriend and I both did our best to make it work, but in the first lockdown our relationship moved on to WhatsApp, and ultimately it forced us apart. But for all the reports of an entire generation permanently blighted by the pandemic, we didn’t have the same experience across the board. My flatmate, aged 24, is nostalgic about the first lockdown, remembering it as a time of sunshine and spring and finishing his dissertation in peace. Another friend said she grew closer with her sister over that time.
It may be that the people I know had the support network and financial prospects to be able to bounce back. But it wasn’t just the lucky ones among us who, looking back now, can see the positives of the pandemic. My friend was living with his elderly father and his brother, who had mental health difficulties at the time. He says it was a “very stressful” time – and yet also “character-building”. During the pandemic he had to be extremely careful about public transport, walking across London instead of taking the tube, even if it took hours.

Young and old: how the Covid pandemic has affected every UK generation
Read more
The subsequent alleviation of risk after the vaccine offered a perspective shift, which had a positive, long-lasting effect on his mental health; he had the realisation of “everything’s fragility”, which he says has helped him. The studies that back this up are in the minority, but they do exist, for example, a systematic review by the BMJ suggests that Covid has had little significant impact on mental health across the population, including in young people. One study from Italy goes even further, reporting that 14- to 20-year-olds had more time for self-discovery and personal growth.
But it’s telling that most of my friends seem to have decided not to mention the pandemic again. For me, that is sufficient proof that it did do some damage. My friends and I don’t reminisce about shared experiences from this time because we don’t have any; it feels like a hole in time. Even the positive reflections are couched in conflicted terms, or apologetic for seeing the good in a traumatic experience. Covid-19 might have stolen a chunk of our adolescence but my peersseem keen to make the best of a bad situation, and a lot of them talk of going through a “second youth” now.
- Isabel Brooks is a freelance writer
Yommie
SpeedLimited
- Oct 2, 2013
- 64,204
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #510
Log in to Facebook
Log in to Facebook to start sharing and connecting with your friends, family and people you know.
 www.facebook.com
www.facebook.com
Log in to Facebook
Log in to Facebook to start sharing and connecting with your friends, family and people you know.
www.facebook.com
Weekly Ontario Update for Friday, March 22, 2024:
This update is very delayed due to recent travel obligations. Unless indicated otherwise, information in this update includes data up until Saturday, March 16, so data is delayed.Data relating to deaths is even further delayed as cause of death is taking MONTHS to be determined. So recent deaths are far WORSE that are reported. NEW! Daily averages are now going to be removed from this update as weekly reporting is typical at this point.
- Recent cases: 897 (+ 178 compared to last week)

Estimates suggest that the actual number of new cases could be more than 10 times higher than what is being reported due to limited eligibility for testing! - Weekly positivity rate: 6.2% (+ 1.1% since last week)
- Recent deaths: 8 (4 FEWER than last week)
- Total deaths: 15 deaths have been added to the total since last week (- 13 fewer compared to last week)
Recent deaths are a lagging indicator of the current level of new cases. Deaths are underreported because they are based on date of death and by the time the cause of death is reported, it is no longer considered recent! - NEW! Average daily hospital bed occupancy (March 3 - March 9): 293* (- 75 since last week week).
*Please interpret the COVID-19 hospitalization data with caution as not all centers are reporting.. - The completeness of COVID-19 hospitalization data, which PHO obtains from the provincial Case and Contact Management database (CCM), has been declining over the course of the 2023-24 surveillance period. PHO is currently working on updates to the ORVT that will include enhancements to respiratory outcome indicators (i.e., hospital bed occupancy), which will help to support surveillance and reporting on COVID-19 outcomes. These updates will be live in the coming weeks.
Sources: Total cases, total deaths, testing levels and wastewater levels: https://www.publichealthontario.ca/.../Respiratory-Virus...
Some additional COVID stats and info: https://twitter.com/MoriartyLab
Users who are viewing this thread
Total: 1 (members: 0, guests: 1)
Pakistan Defence Latest
Country Watch Latest
Latest Posts
-

-
 Hezbollah-Israel Conflict 2024 - Lebanon & Occupied Palestine Territories (54 Viewers)
Hezbollah-Israel Conflict 2024 - Lebanon & Occupied Palestine Territories (54 Viewers)- Latest: Dalit
-
-