Navigation
Install the app
How to install the app on iOS
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
More options
Style variation
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Covid-19 News and Discussions
- Thread starter Yommie
- Start date
Yommie
SpeedLimited
- Oct 2, 2013
- 64,203
- 37,191
- Country of Origin

- Country of Residence

- Thread starter
- #602
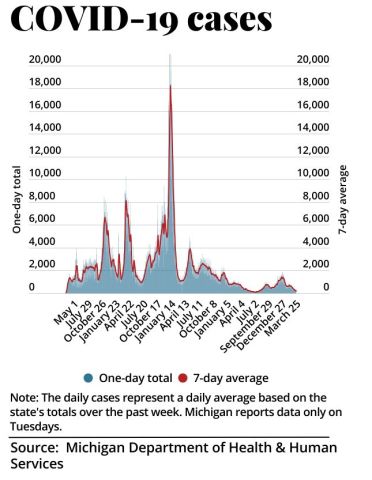
COVID Tracker | COVID cases stable, deaths fall | Bridge Michigan
This continuously updated tracker shows Michigan's COVID-19 case numbers, positivity rate, county infection rates, and weekly cases along with maps and daily state curve data.
COVID Tracker | COVID cases stable, deaths fall
April 9, 2024Last updated: Tuesday, April 9, at 4:18 p.m. This post will be continuously updated with Michigan coronavirus locations and updated COVID-19 news.
For more interactive maps and charts, see the Michigan Coronavirus Dashboard, showing vaccine distribution information, case numbers, locations, deaths and demographics.
Michigan public health officials reported 1,458 confirmed and probable COVID-19 cases for the week ending Tuesday, down slightly from the 1,463 reported last week.
The state reported 30 additional deaths for the week ending Tuesday, down from the 36 reported April 2.
The number of confirmed COVID-19-positive hospital patients fell Monday to 233, down from 247 a week earlier.
Related: Whitmer book spurs president talk, joins list of Michigan political reads
Experts say that state-reported cases are likely a vast undercount because many people either no longer test for the virus when they have symptoms or rely on home tests.— Mike Wilkinson
Yommie
SpeedLimited
- Oct 2, 2013
- 64,203
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #603

Dispute over COVID-19 social distancing led to murder at Toronto LCBO
The judge found that Michael Roberts, 23, killed 21-year-old Jakub Sudomericky in an LCBO parking lot following a “brief verbal altercation” over distancing at the checkout.
 www.thestar.com
www.thestar.com
Dispute over COVID-19 social distancing led to murder at Toronto LCBO
The judge found that Michael Roberts, 23, killed 21-year-old Jakub Sudomericky in an LCBO parking lot following a “brief verbal altercation” over distancing at the checkout.Updated 8 hrs ago
April 12, 2024
1 min read
Save

Jakub Sudomericky, 21.
Toronto police

By Jacques GallantCourts and Justice Reporter
A dispute over social distancing at a Toronto LCBO in 2020 ultimately led to a man being convicted Friday of second-degree murder.
Superior Court Justice Nola Garton found that 23-year-old Michael Roberts “knowingly and willingly engaged” 21-year-old Jakub Sudomericky in the liquor store parking lot after the two had a “brief verbal altercation” over distancing at the checkout at the height of the COVID-19 pandemic, in which the judge said Sudomericky was the “aggressor.”
Roberts, who was armed that day with a loaded handgun, had already admitted to fatally shooting Sudomericky and pleaded guilty to manslaughter, but the plea was rejected by the Crown.
ARTICLE CONTINUES BELOW
He testified in the judge-alone trial that Sudomericky provoked him in the parking lot of the LCBO on Danforth Ave. near Victoria Park Ave. on a Sunday afternoon in October 2020, calling him a “f—-ing” n-word and pulling a knife on him.
Roberts said this caused him to go into a “blind rage,” take out his gun and chase after Sudomericky before shooting him.
The Crown argued that Roberts “wasn’t a credible witness,” was not provoked, and that no slur was uttered. Even if one was said, it would not be enough for a provocation defence, prosecutors said.
The defence argued that the “cumulative effect” of the provocation, in combination with the effects of the multiple joints of marijuana Roberts had smoked prior to the incident, prevented him from forming the necessary intent to commit murder.
Garton gave only brief reasons Friday morning in convicting Roberts, saying a lengthy ruling will be released later. Roberts, sitting in the prisoner’s box in a grey shirt and blazer, showed no emotion as he was convicted.
ARTICLE CONTINUES BELOW
“Having considered all of the evidence, including the video evidence, and the submissions of counsel, I find that the Crown has established beyond a reasonable doubt that the defence of provocation does not apply in this case,” she said.
Garton also found that Roberts was not impaired and intended to shoot and kill Sudomericky, or cause him serious injuries that he knew would likely cause death. “I therefore find Mr. Roberts guilty of second-degree murder.”
The conviction carries an automatic life sentence, but a judge will have to decide after a sentencing hearing how long Roberts must serve in prison before becoming eligible for parole, a period between 10 and 25 years.
That judge will not be Garton, whose last day in the courtroom ahead of her retirement from the bench was Friday.
The case has been adjourned until May.
Yommie
SpeedLimited
- Oct 2, 2013
- 64,203
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #610
Hidden Long COVID crisis deepens in New Zealand
With a new COVID surge circulating unchecked in the country, the dangers and consequences of Long COVID are being underplayed by the political establishment.
www.wsws.org
Hidden Long COVID crisis deepens in New Zealand
John Braddock
9 April 2024
February 28 marked four years since COVID-19 was first reported in New Zealand. Today, the virus is still circulating, with new strains, including the more infectious variants like JN.1, having arrived two years after the Omicron variant became widespread.Initially, with strict border controls and lockdowns imposed by the Jacinda Ardern-led Labour Party government, New Zealand was largely successful keeping the pandemic at bay.
However, under pressure from big business and the media, Ardern abandoned the government’s elimination policy in late 2021 and adopted the criminal “let it rip” agenda that has killed more than 27.4 million people globally. Last year Ardern’s successor, Chris Hipkins, announced the formal end of all remaining public health measures.
The policy has been reinforced by the recently installed far-right National Party led coalition government. Health NZ last month declared that household contacts of people with COVID-19 no longer need to test daily unless they develop symptoms. Rapid antigen tests (RATs) will likely only be available free until June, with the government non-committal about paying for more.
On April 2, Health NZ declared that 3,399 new cases, of which 67 percent were reinfections, had been reported the previous week, with seven more deaths attributed to the virus. Nationwide wastewater readings suggest that the real number of cases is twice as high.
Despite ongoing attempts by the political establishment to convince the population that the COVID pandemic is “over” or no worse than seasonal influenza, in 2023 the coronavirus caused more than 12,000 hospitalisations and 1,000 deaths.
Total deaths in New Zealand attributed to COVID will pass 4,000 this week, but the real toll is likely higher. According to Health NZ there are 226 deaths that may or may not be COVID-related, and 1,773 people who died shortly after being infected with COVID, but whose deaths have been deemed unrelated to COVID.
Otago University epidemiologist Michael Baker warned in the Conversation last month that a fifth wave of the virus, which entered the country during the summer, was significantly larger than the fourth wave, signaling that “we cannot rely on the comforting assumption that COVID will get less severe over time.” Baker condemned the “growing pandemic complacency” from political leaders and sections of the public.
The government is doing its best to bury any evidence of the ongoing dangers. Last week Health Minister Shane Reti and Finance Minister Nicola Willis falsely claimed that they had established a Long COVID expert advisory group as part of the government’s response. Health NZ was forced to reveal the group was actually established in 2022 but disestablished the same year.
Baker and colleagues, including Amanda Kvalsvig (Otago University) and Matire Harwood (Auckland University) are meanwhile turning their attention to the “undercounting” of Long COVID.
International evidence indicates that between 5 to 15 percent of all infections can lead to Long COVID, which can persist for up to four years, with symptoms that fluctuate from mild to severe. With every re-infection, the chances of developing Long COVID increase, and there is no known cure.
Some of the most prevalent symptoms of Long COVID
According to the New Zealand researchers, there are more than 200 individual symptoms linked to Long COVID, with the dominant ones being fatigue and brain fog. While some are mild and transient, other effects can be life-altering, including heart attacks, strokes, diabetes, chronic fatigue syndrome and a range of neurological effects.
Baker said in a Radio NZ interview that Long COVID can be damaging to the “entire population,” and can affect the brain development of children and teenagers. It can also impact on foetuses. In response, Minister Nicola Willis flatly said the government would not commit to adopting any minimum standards to prevent it.
According to Professor Kvalsvig, teachers are the most vulnerable occupation to getting COVID, and therefore Long COVID, followed by healthcare workers. Some who had the virus early in 2020 are still not well. “So the experience of being not listened to and not believed has been very harmful for them alongside the very considerable health impacts that they’ve had from Long COVID,” she said.
Culpability for the dire situation in schools rests with the teacher unions, the NZ Educational Institute (NZEI) and Post-Primary Teachers Association (PPTA). Both opposed demands to close the schools when the pandemic first hit, and assisted in reopening them after Labour ended the zero-COVID policy.
Neither union has mounted any campaign, or called strike action, to protect the health and safety of teachers and students. Nor have they raised any demands for nationwide protections, such as the provision of air filters, to minimise in-school impacts.
In a sign of the measures that will be used in workplaces, hospitals and elsewhere, Associate Education Minister David Seymour—the leader of the far-right ACT Party—recently declared that parents should send sick children to school in the name of combating a so-called “truancy crisis.” Seymour stated last week: “As we move out of a COVID period—or have moved out of a COVID period—we’ve got to look at other challenges we face like not enough kids going to school.”
MEHRING BOOKS
COVID, Capitalism, and Class War: A Social and Political Chronology of the Pandemic
A compilation of the World Socialist Web Site's coverage of this global crisis, available in epub and print formats.
BUY YOUR COPY TODAY
This criminal policy has nothing to do with helping children learn. The aim is to ensure that parents keep working without being interrupted to care for their sick children.
Presenters to a webinar on April 3 titled “Long COVID—Are we taking it seriously enough?” organised by the Helen Clark Foundation, said that a Long COVID registry, established in July last year, showed that most sufferers were in the mid-40s age bracket, often needing to work while looking after households. Most were healthy before COVID. Researcher Paula Lorgelly said many now have a quality of life similar to patients suffering cancer and multiple sclerosis.
Patient advocate Jenene Crossan said that because of the absence of “bio-markers,” large numbers of people do not even know they have Long COVID. Trying to get a diagnosis was like the “wild west,” and doctors lacked the time and resources to deal with chronic conditions.
Baker warned that schools and workplaces are “cutting corners” on safety. He called for a “massive cultural shift,” saying it should not be regarded as “normal” to get multiple respiratory infections “over and over again.” The government needed to “take the leadership” and insist such a situation is “intolerable,” Baker said.
However Baker, who was a Labour government advisor, well knows that the perspective of trying to pressure any government has proven to be a dead end. When Labour abandoned its elimination policy and subsequent health protections it did so against the advice of the vast majority of public health experts.
The National-ACT-NZ First government has already made its intentions clear. With hospitals facing overcrowding, understaffing and a lack of resources, vital funding is being cut. Last week the Health Ministry announced 134 jobs would be axed as it seeks to slash its budget by $78 million by 2025.
The attitude of New Zealand’s ruling elite to the lives and well-being of the working class was summed up by ACT Party MP and Minister for Workplace Relations Brooke Van Velden, who blurted out last year when she was the party health spokesperson: “When it came to COVID, we completely blew out what the value of a life was, completely, I’ve never seen such a high value on life.”
A strategy to eliminate COVID-19, which is an international issue, includes mass testing, contact tracing, the safe isolation and treatment of infected patients, the universal use of high-quality masks, and the provision of clean indoor air. There must be a vast expansion in funding for Long COVID research and a systematic program of scientific education.
Such a strategy, however, will never be implemented under capitalism, which subordinates all public health spending to the insatiable profit interests of the financial oligarchy. It requires a turn to the working class and the building of a mass socialist movement fighting to restructure society on the basis of social need, not private profit.
Yommie
SpeedLimited
- Oct 2, 2013
- 64,203
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #611
COVID-19: Current cases – Health New Zealand | Te Whatu Ora
Read the latest information about confirmed and probable cases of COVID-19 in New Zealand.
 www.tewhatuora.govt.nz
www.tewhatuora.govt.nz
COVID-19 cases summary
| New case average* | RATs uploaded average* |
| 483 ↓ | 584 ↑ |
| Cases in hospital as at midnight Sunday | Cases in ICU as at midnight Sunday |
| 145 | ** |
| Deaths attributed to COVID* | Total deaths attributed COVID |
| 2 ↑ | 3,936 |
** Not currently available
Current situation
Summary| In the last week | New cases reported | 3385 |
|---|---|---|
| Reinfections | 2109 | |
| Reinfections (< 90 days) | 37 | |
| Total since first New Zealand case | Cases reported | 2624496 |
| Reinfections | 356816 | |
| Reinfections (< 90 days) | 26294 |
Case outcomes since first New Zealand case
| COVID-19 cases | Change in the last week | Total |
|---|---|---|
| Recovered | 3391 | 2617182 |
| Deceased* | 13 | 3936* |
Deaths with COVID-19
| Cause of death | Died within 28 days of positive test | Died more than 28 days after positive test | Total | Change in the last week |
|---|---|---|---|---|
| COVID as underlying | 2345 | 122 | 2467 | 5 |
| COVID as contributory | 1363 | 106 | 1469 | 8 |
| COVID-attributed total | 3708 | 228 | 3936 | 13 |
| Not COVID | 1782 | 0* | 1782 | 9 |
| Not available | 232 | 0 | 232 | 6 |
| Total | 5722 | 228 | 5950 | 28* |
Of the 28 people whose deaths we are reporting today: two were from Northland, six were from Auckland region, five were from Waikato, one was from Hawke's Bay, one was from Taranaki, five were from Wellington region, four were from Canterbury, three were from Southern, one was unknown.
One was in their 30s, three were in their 50s, one was in their 60s, nine were in their 70s, five were in their 80s and nine were aged over 90. Of these people, 13 were women and 15 were men.
Case details
Number of active cases| Change in the last week | Total since first NZ case | |
|---|---|---|
| Confirmed | 3228 | 2580385 |
| Probable | 157 | 44111 |
| Total | 3385* | 2624496 |
Definitions
| Active case - confirmed | Confirmed cases are people who have received a positive PCR test OR someone who has received a positive result on a Rapid Antigen Test. For more details, see the COVID-19 case definition. |
|---|---|
| Active case - probable | A probable case is when someone is diagnosed based on their exposure to other people with COVID-19 and on their symptoms. |
| Reinfections | Reinfections are cases in an individual who reported a case 29 or more days previously. |
| Recovered | Recovered cases are people who had the virus, where at least 7 days have passed since their symptoms started and they have not had symptoms for 72 hours, and they have been cleared by the health professional responsible for their monitoring. |
| Deceased | Includes all deaths where COVID-19 is determined to have been the underlying cause of death or a contributory cause of death. |
Cases reported each day
Daily confirmed and probable cases

This graph shows the count of all cases of COVID-19 every day (all cases – confirmed and probable) since the first New Zealand case in late February 2020. The graph shows the rapid increase of daily cases from mid-February 2022 to early March 2022, driven by the Omicron variant. From mid-March to mid-April 2022, cases rapidly declined, followed by a period of slower decline until early July. This was followed by a rapid increase in cases, peaking in August before a steady decline in new daily cases. Reported new daily cases hit their lowest since February 2022 in September 2022.
New COVID-19 cases reported each day
This graph shows the count of all cases of COVID-19 every day (all cases – confirmed and probable) since the first New Zealand case in late February 2020. The graph shows the rapid increase of daily cases from mid-February 2022 to early March 2022, driven by the Omicron variant. From mid-March to mid-April 2022, cases rapidly declined, followed by a period of slower decline until early July. This was followed by a rapid increase in cases, peaking in August before a steady decline in new daily cases. Reported new daily cases hit their lowest since February 2022 in September 2022.
COVID-19 by location
Total cases by location

This bar graph shows the total cases and their status by health district and those with recent travel history.
The ‘At the border’ data group includes cases detected in managed isolation or quarantine facilities from the period when these were operating, as well as cases with recent travel history from after that time. They are not included in the district totals. Before 17 June, people in managed isolation or quarantine facilities were included in the total of the relevant district.
Total COVID-19 cases by location graph
This graph shows:
- This bar graph shows the total cases and their status by health district and those with recent travel history.
The ‘At the border’ data group includes cases detected in managed isolation or quarantine facilities from the period when these were operating, as well as cases with recent travel history from after that time. They are not included in the district totals. Before 17 June, people in managed isolation or quarantine facilities were included in the total of the relevant district.
Total cases by location
| Location | Active | Recovered | Deceased | Total | New cases in the last week |
|---|---|---|---|---|---|
| Auckland | 210 | 246509 | 265 | 246984 | 209 |
| Bay of Plenty | 158 | 115124 | 183 | 115465 | 158 |
| Canterbury | 541 | 346590 | 547 | 347678 | 540 |
| Capital and Coast | 298 | 185659 | 176 | 186133 | 300 |
| Counties Manukau | 291 | 293166 | 318 | 293775 | 294 |
| Hawke's Bay | 78 | 86161 | 168 | 86407 | 78 |
| Hutt Valley | 130 | 90792 | 98 | 91020 | 130 |
| Lakes | 58 | 51403 | 111 | 51572 | 58 |
| Mid Central | 152 | 96670 | 206 | 97028 | 152 |
| Nelson Marlborough | 139 | 79699 | 156 | 79994 | 139 |
| Northland | 121 | 81192 | 144 | 81457 | 121 |
| South Canterbury | 45 | 34747 | 44 | 34836 | 45 |
| Southern | 306 | 192539 | 373 | 193218 | 307 |
| Tairāwhiti | 22 | 26653 | 44 | 26719 | 22 |
| Taranaki | 86 | 65805 | 128 | 66019 | 86 |
| Unknown | 3 | 2270 | 9 | 2282 | 4 |
| Waikato | 263 | 208697 | 391 | 209351 | 264 |
| Wairarapa | 48 | 25616 | 64 | 25728 | 48 |
| Waitematā | 356 | 310228 | 405 | 310989 | 357 |
| West Coast | 29 | 15835 | 22 | 15886 | 29 |
| Whanganui | 44 | 34535 | 78 | 34657 | 44 |
| At the Border* | 0 | 27292 | 6 | 27298 | NA |
| Total | 3378 | 2617182 | 3936 | 2624496 | 3385 |
You can also view a detailed breakdown of daily case numbers for each district since the beginning of the pandemic by clicking the ‘download’ button on the right hand side of this page: New Zealand COVID-19 data.
Note: we cannot give detailed information about cases in your district, city or town, as we must protect the privacy of the people concerned.
Also in this section
Last updated: 8 April 2024Yommie
SpeedLimited
- Oct 2, 2013
- 64,203
- 37,191
- Country of Origin
- Country of Residence
- Thread starter
- #615
Study reveals how SARS-CoV-2 hijacks lung cells to drive COVID-19 severity
Researchers identified how SARS-CoV-2 targets and manipulates specific lung cells, using innovative techniques to trace the virus's impact on the cells' gene expression, revealing insights into early COVID-19 pathogenesis.
 www.news-medical.net
www.news-medical.net
Study reveals how SARS-CoV-2 hijacks lung cells to drive COVID-19 severity


In a recent study published in the Journal of Experimental Medicine, researchers identified the cellular tropism and transcriptome consequences of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) by infecting human lung tissue and using single-cell ribonucleic acid sequencing (scRNA-seq) to rebuild the transcriptional program in "infection pseudotime" for distinct lung cell types.
Lower respiratory infections, such as coronavirus disease 2019 (COVID-19), are a leading cause of death worldwide, producing pneumonia and acute respiratory distress syndrome. Understanding their early phases is difficult. Researchers used classical histopathological approaches and single-cell multi-omic profiling to infer early phases in human pathogenesis from lung lavage, biopsy, or autopsy materials. These approaches reveal a thorough picture of COVID-19 pneumonia at unparalleled cellular and molecular resolution, implying infection models including alveolar epithelium, capillaries, macrophages, and myeloid cells.
Study: Interstitial macrophages are a focus of viral takeover and inflammation in COVID-19 initiation in human lung. Image Credit: Dotted Yeti / ShutterstockAbout the study
In the present study, researchers developed an experimental COVID-19 model to investigate early molecular processes and pathogenic mechanisms of SARS-CoV-2 infection at the cellular level in native tissues of the human lung.The researchers established SARS-CoV-2's cellular tropism and its unique and dynamic impacts on host cellular gene expression in specific types of lung cells. Prominent targets were lung-resident macrophages, of which one SARS-CoV-2 takes over transcriptomes, inducing a targeted host interferon (IFN) antiviral program, and several chemokines and pro-fibrotic and pro-inflammatory and cytokines signaling to various structural and immunological cells of the lung.
To determine the early stages of COVID-19 in human lungs, the researchers sliced lung tissue obtained from surgical specimens or organ donor individuals into thick sections and used them for tissue culture analysis. Subsequently, they exposed the tissues to the SARS-CoV-2 USA-WA1 2020 strain at 1.0 multiplicity of infection (MOI) for two hours before allowing the SARS-CoV-2 infection to continue for two to three days. They performed a plaque test on culture supernatants.
The researchers separated the slices and examined them by scRNA-seq to evaluate host and viral genetic expression during the SARS-CoV-2 infection. They also examined the viral RNA molecules' junctional structure and processing by analyzing the scRNA-seq dataset with the SICILIAN framework. They used molecular atlas markers to distinguish lung cell types in healthy lung slices and measure viral RNA levels in infected cells.
The team performed multiplexed single-molecule fluorescence in situ hybridization (smFISH) to confirm lung cell tropism findings and show infected cells. They used single-cell gene expression patterns to identify cellular targets for inflammatory and pro-fibrotic signals elicited by the SARS-CoV-2 infection of a-IMs. They devised a technique for purifying macrophage populations from human lungs with a SARS-CoV-2 spike (S) protein-pseudotyped lentivirus (lenti-S-NLuc-tdT) to investigate lung macrophage entrance routes.
The researchers productively infected human lung slices cultivated ex vivo with SARS-CoV-2, with production rising between 24 and 72 hours of culture. They heat-inactivated, ultraviolet (UV)-treated, or administered 10.0 µM remdesivir, an RNA-dependent RNA polymerase inhibitor used as a COVID-19 therapeutic, to prevent viral stock infection.
Results
The analysis showed that SARS-CoV-2 preferentially infects active interstitial macrophages (IMs), which can amass hundreds of SARS-CoV-2 RNA molecules, comprising >60% of the cell transcriptome and producing dense viral RNA bodies. Infected alveolar macrophages (AMs) exhibit no severe reactions, with spike (S) protein-dependent viral entrance into AMs utilizing angiotensin-converting enzyme 2 (ACE2) and the cluster of differentiation 169 (CD169) and IM entry via CD209.They found canonical sub-genomic junctions between the unusual sequence reads beyond their 39 terminal regions, indicating canonical-type SARS-CoV-2 messenger RNA (mRNA) production in the pulmonary cultures. They also found hundreds of new subgenomic junctions, showing a wide range of non-canonical and canonical sub-genomic SARS-CoV-2 RNAs produced during pulmonary infection.
 Model of COVID-19 initiation in the human lung and transition from viral pneumonia to lethal COVID-19 ARDS. (a) SARS-CoV-2 virion dissemination and arrival in the alveoli. Luminal AM encounter virions shed from the upper respiratory tract that enter the lung. AMs can express low to moderate numbers of viral RNA molecules and can propagate the infection but “contain” the viral RNA from taking over the total transcriptome and show only a very limited host cell inflammatory response to viral infection. (b) Replication and epithelial injury. SARS-CoV-2 virions enter AT2 cells through ACE2, its canonical receptor, and “replicate” to high viral RNA levels, producing infectious virions and initiating viral pneumonia. (c) a-IM takeover and inflammation signaling. SARS-CoV-2 virions spread to the interstitial space through either transepithelial release of virions by AT2 cells or injury of the epithelial barrier, and enter a-IMs. Infected a-IMs can express very high levels of viral RNA that dominate (“take over”) the host transcriptome and can propagate the infection. Viral takeover triggers induction of the chemokines and cytokines shown, forming a focus of inflammatory and fibrotic signaling. (d) Endothelial breach and immune infiltration. The a-IM inflammatory cytokine IL6 targets structural cells of the alveolus causing epithelial and endothelial breakdown, and the inflammatory cytokines recruit the indicated immune cells from the interstitium or bloodstream, which flood and infiltrate the alveolus causing COVID-19 ARDS. Local inflammatory molecules are amplified by circulating immune cells, and reciprocally can spread through the bloodstream to cause systemic symptoms of cytokine storm. (e) Comparison of the SARS-CoV-2 viral lifecycle in AMs and IMs. Although both can produce infectious virions, note differences in viral entry receptors (AMs can use ACE2 and CD169/SIGLEC1, whereas IMs use CD209); viral RNA transcription of dsRNA intermediates (greater in AMs); replication of full-length genomic RNA (greater in IMs); viral takeover, formation of RNA bodies, and induction of a robust host cell inflammatory response (only in IMs), and cell destruction/death (only in IMs).")
 Cell Density eBook - What are the Many Applications of Cell Density Sensors? eBook This eBook discusses the many applications of cell density sensors and how innovative methods can improve the monitoring of cell density.Download the latest edition
Cell Density eBook - What are the Many Applications of Cell Density Sensors? eBook This eBook discusses the many applications of cell density sensors and how innovative methods can improve the monitoring of cell density.Download the latest editionHeat, UV-C inactivation, or remdesivir therapy prevented the development of canonical and non-canonical connections. The team observed SARS-CoV-2 takeover of an activated IM subtype in 176,382 cells with high-quality transcriptomes obtained from infected lung slices of four donor lungs and in 112,359 cells from mock-infected slices (cultured without viral addition) and 95,389 uncultured control cells (directly from freshly cut lung slices). A differential gene expression study of a-IMs over infection pseudotime revealed host gene expression alterations corresponding to SARS-CoV-2 RNA levels.
The study found that COVID-19 pneumonia infection and takeover cause an early antiviral cell response specific to activated interstitial macrophages, resulting in a powerful immunological and fibrotic signaling center. Inflammasome activation is uncommon and only detectable late in a-IM infection. Blocking antibodies against CD169 and CD209 prevented entrance into IMs and AMs. The study also highlighted IMs as the most vulnerable lung target, with initial emphasis on inflammation and fibrosis. Two unique molecular lineages of macrophage targets react differently to SARS-CoV-2, influencing etiology and treatments.
Users who are viewing this thread
Total: 1 (members: 0, guests: 1)
Pakistan Defence Latest
-

-

-

-
 Breaking news: Malakand 10 diplomates from different countries attacked...All safe (1 Viewer)
Breaking news: Malakand 10 diplomates from different countries attacked...All safe (1 Viewer)- Latest: hussain0216
Country Watch Latest
-

-

-
Dr. Shahiduzzaman: in order to change India’s habitual perception, our only answer as I feel is nuclearization. (5 Viewers)
- Latest: Chandragupt Maurya
-
-
Latest Posts
-
 Hindutva Lobby Flexes its Muscle in California by Brofessor Riazul Haq sb (2 Viewers)
Hindutva Lobby Flexes its Muscle in California by Brofessor Riazul Haq sb (2 Viewers)- Latest: Guru Dutt
-

-
-
'Indus Water Treaty Not feasible to maintain': India serves notice to Pakistan, seeks Modification. (14 Viewers)
- Latest: Chandragupt Maurya
-